

Casting in finger trap traction without reduction versus closed reduction and percutaneous pin fixation of dorsally displaced, over-riding distal metaphyseal radius fractures in children under 11 years old: a study protocol of a randomised controlled trial
- PMID: 34039573
- PMCID: PMC8160196
- DOI: 10.1136/bmjopen-2020-045689
Casting in finger trap traction without reduction versus closed reduction and percutaneous pin fixation of dorsally displaced, over-riding distal metaphyseal radius fractures in children under 11 years old: a study protocol of a randomised controlled trial
Abstract
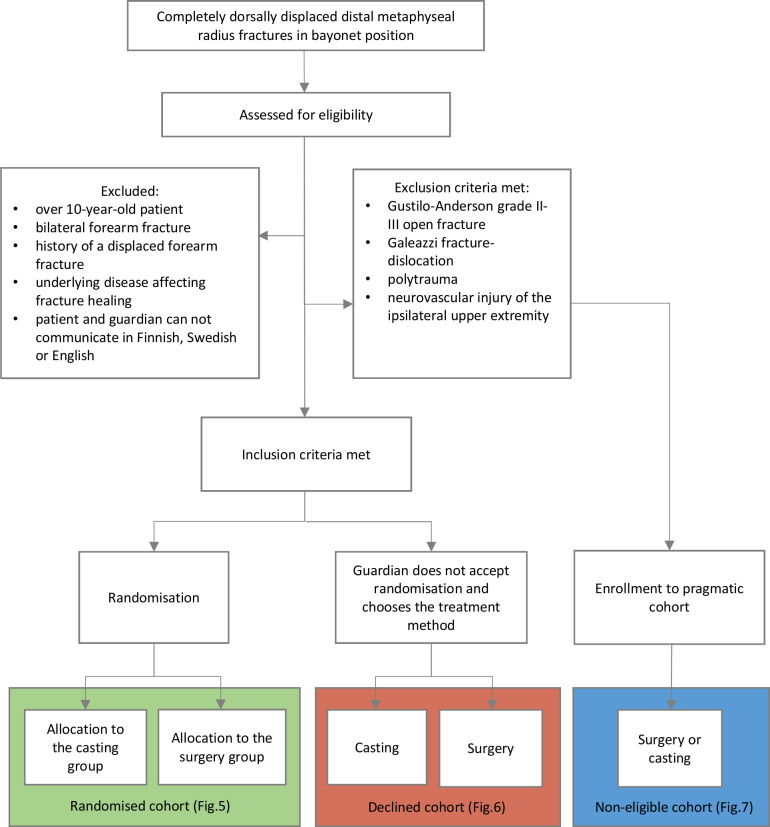
Introduction: Distal radius is the most common site of fracture in children, comprising 23%-31% of all paediatric fractures. Approximately one-fifth of these fractures are displaced. Completely displaced distal metaphyseal radius fractures in children have traditionally been treated with closed reduction. Recent evidence suggests that correcting the shortening in over-riding distal metaphyseal radius fractures is not necessary in prepubertal children. To date, no published randomised controlled trial (RCT) has compared treatment of these fractures in children by casting the fracture in bayonet position to reduction and pin fixation.
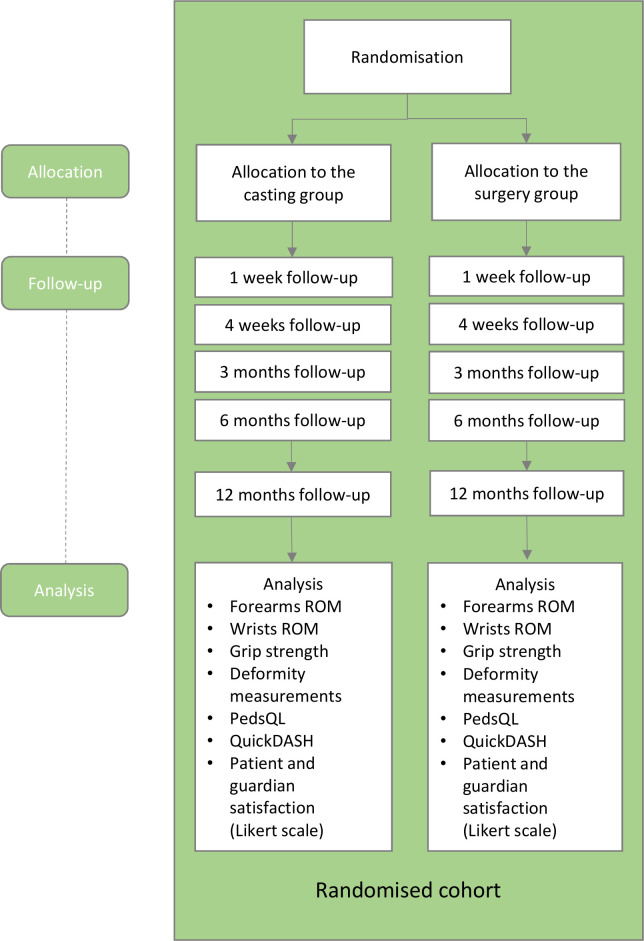
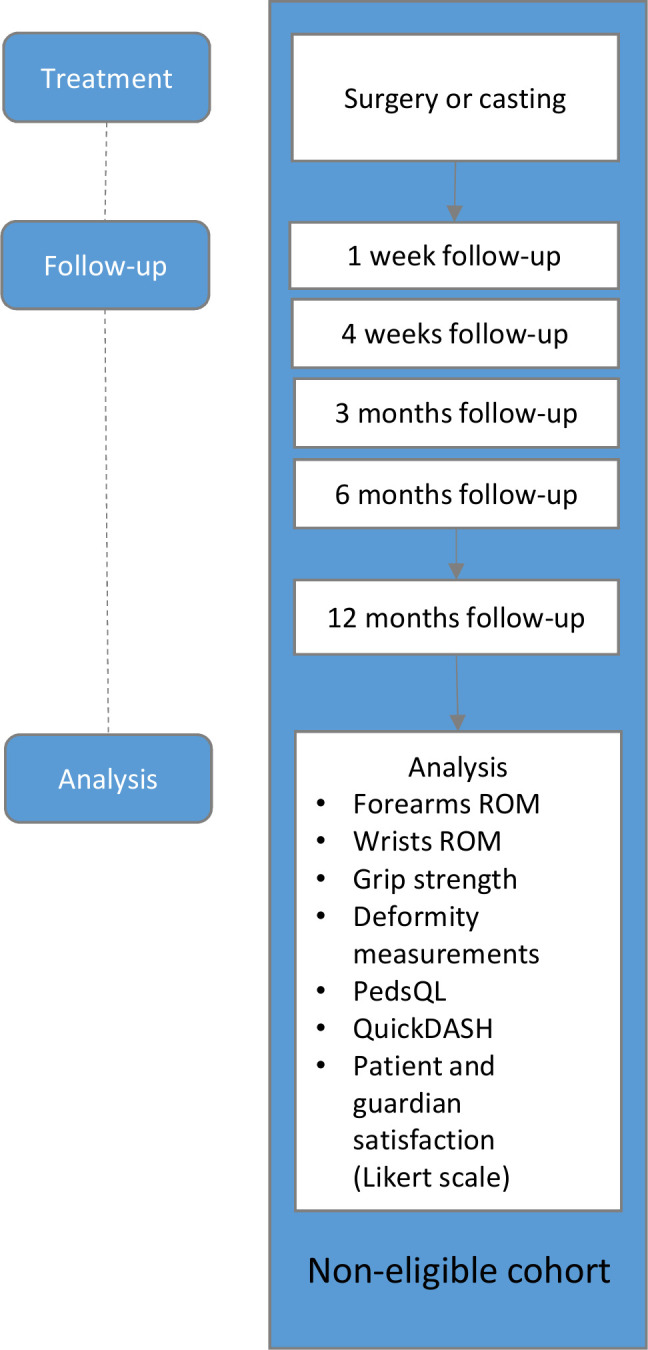
Methods and analysis: We will conduct an RCT to compare the outcomes of casting the fracture in bayonet position in children under 11 years of age to reduction and percutaneous pin fixation. 60 patients will be randomly assigned to casting or surgery groups. We have two primary outcomes. The first is ratio (injured side/non-injured side) in the total active forearm rotation and the second is ratio (injured side/non-injured side) in total active range of motion of the wrist in the flexion-extension plane at 6 months. The secondary outcomes will include axial radiographic alignment, passive extension of the wrists, grip strength and length of forearms and hands, patient-reported outcome QuickDASH and pain questionnaire PedsQL. Patients not willing to participate in the RCT will be asked to participate in a prospective cohort. Patients not eligible for randomisation will be asked to participate in a non-eligible cohort. These cohorts are included to enhance the external validity of the results of the RCT. Our null hypothesis is that the results of the primary outcome measures in the casting group are non-inferior to surgery group.
Ethics and dissemination: The institutional review board of the Helsinki and Uusimaa Hospital District has approved the protocol. We will disseminate the findings through peer-reviewed publications.
Trial registration number: NCT04323410.
Protocol: V.1.1, 29 September 2020.
Keywords: orthopaedic & trauma surgery; paediatric orthopaedic & trauma surgery; paediatric surgery; trauma management.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures




Similar articles
-
Is casting of displaced paediatric distal forearm fractures non-inferior to reduction under general anaesthesia? Study protocol for a pragmatic, randomized, controlled non-inferiority multicentre trial (the casting trial).Trials. 2024 Jun 27;25(1):420. doi: 10.1186/s13063-024-08253-z. Trials. 2024. PMID: 38937792 Free PMC article.
-
Effectiveness and cost-effectiveness of surgery versus casting for elderly patients with Displaced intra-Articular type C distal Radius fractures: protocol of a randomised controlled Trial with economic evaluation (the DART study).BMJ Open. 2022 Apr 1;12(4):e051658. doi: 10.1136/bmjopen-2021-051658. BMJ Open. 2022. PMID: 35365511 Free PMC article.
-
Surgical fixation with K-wires versus plaster casting in the treatment of dorsally displaced distal radius fractures: protocol for Distal Radius Acute Fracture Fixation Trial 2 (DRAFFT 2).BMJ Open. 2019 Mar 23;9(3):e028474. doi: 10.1136/bmjopen-2018-028474. BMJ Open. 2019. PMID: 30904879 Free PMC article.
-
Percutaneous pinning for treating distal radial fractures in adults.Cochrane Database Syst Rev. 2020 Feb 7;2(2):CD006080. doi: 10.1002/14651858.CD006080.pub3. Cochrane Database Syst Rev. 2020. PMID: 32032439 Free PMC article.
-
Are Volar Locking Plates Superior to Percutaneous K-wires for Distal Radius Fractures? A Meta-analysis.Clin Orthop Relat Res. 2015 Sep;473(9):3017-27. doi: 10.1007/s11999-015-4347-1. Epub 2015 May 16. Clin Orthop Relat Res. 2015. PMID: 25981715 Free PMC article. Review.
Cited by
-
Pediatric distal both-bone forearm fractures treated with percutaneous pinning with or without ulna fixation: a retrospective cohort study from two centres.BMC Musculoskelet Disord. 2024 Aug 29;25(1):683. doi: 10.1186/s12891-024-07822-2. BMC Musculoskelet Disord. 2024. PMID: 39210474 Free PMC article.
-
Casting Without Reduction Versus Closed Reduction With or Without Fixation in the Treatment of Distal Radius Fractures in Children: Protocol for a Randomized Noninferiority Trial.JMIR Res Protoc. 2022 Apr 14;11(4):e34576. doi: 10.2196/34576. JMIR Res Protoc. 2022. PMID: 35436224 Free PMC article.
-
Is casting of displaced paediatric distal forearm fractures non-inferior to reduction under general anaesthesia? Study protocol for a pragmatic, randomized, controlled non-inferiority multicentre trial (the casting trial).Trials. 2024 Jun 27;25(1):420. doi: 10.1186/s13063-024-08253-z. Trials. 2024. PMID: 38937792 Free PMC article.
-
Distal radius fractures in children aged 5-12 years: a Swedish nationwide register-based study of 25 777 patients.BMC Musculoskelet Disord. 2023 Jul 10;24(1):560. doi: 10.1186/s12891-023-06680-8. BMC Musculoskelet Disord. 2023. PMID: 37430230 Free PMC article.
-
Health-Related Quality of Life after Fractures of the Distal Forearm in Children and Adolescents-Results from a Center in Switzerland in 432 Patients.Children (Basel). 2022 Sep 28;9(10):1487. doi: 10.3390/children9101487. Children (Basel). 2022. PMID: 36291423 Free PMC article.
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical