

Management of pineal and colloid cysts
- PMID: 34039752
- PMCID: PMC8327315
- DOI: 10.1136/practneurol-2020-002838
Management of pineal and colloid cysts
Abstract
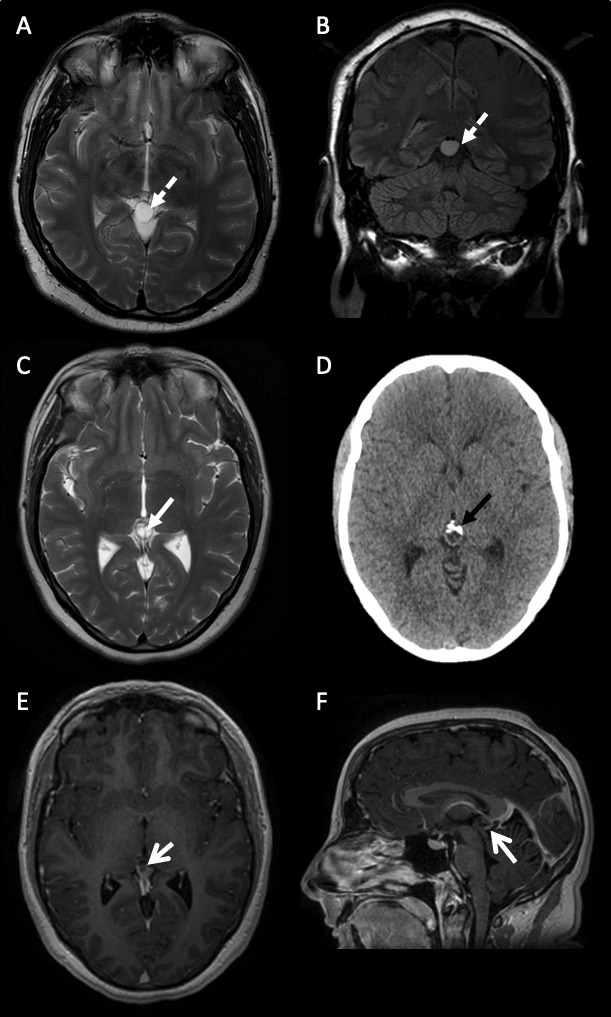
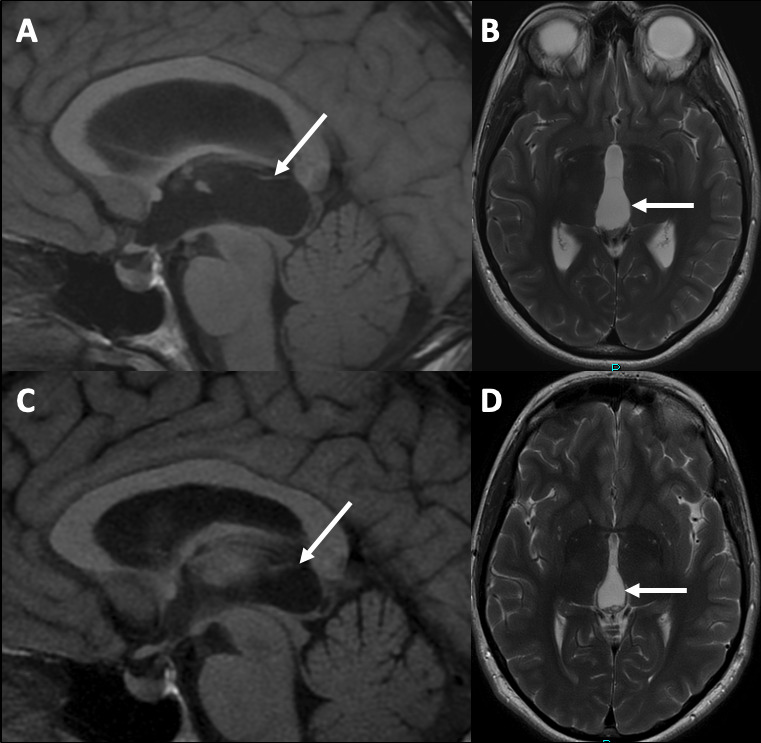
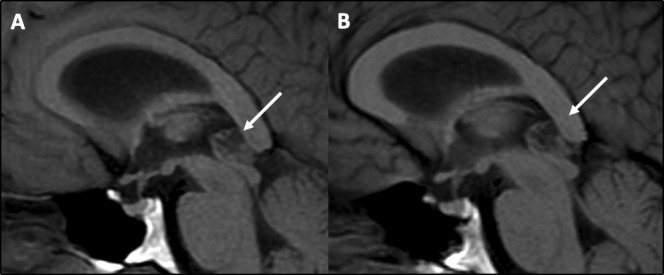
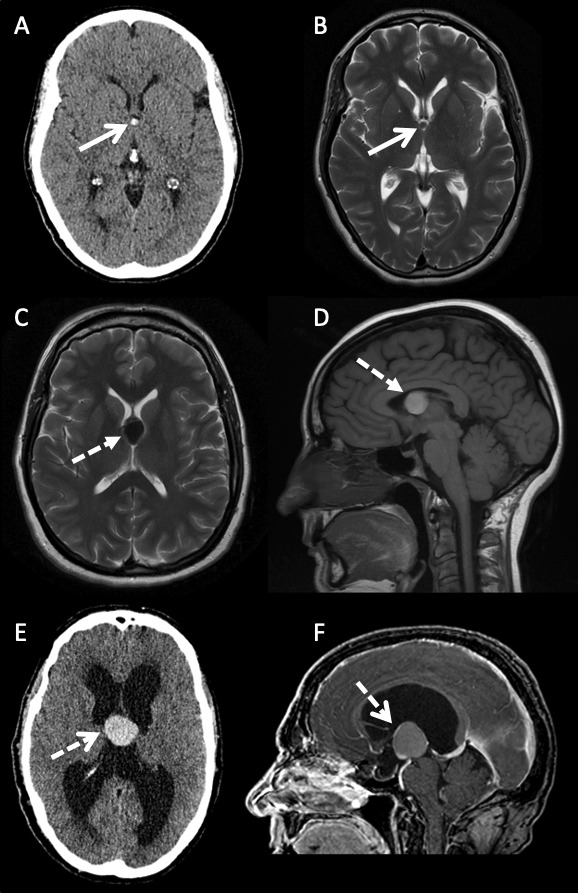
The widespread use of MRI has led to the increasingly frequent diagnosis of pineal and colloid cysts. While most are small and incidental, do not require long-term monitoring and will never need treatment, they are a cause of patient anxiety and clinician uncertainty regarding the optimal management-particularly for larger cysts or those with an atypical appearance. Occasionally pineal cysts, and more commonly colloid cysts, cause hydrocephalus that requires urgent neurosurgical treatment. More recently the non-hydrocephalic symptomatic pineal cyst has been described in the neurosurgical literature but there is controversy over this entity and its management. This review addresses the difficulties in managing pineal and colloid cysts and provides a pragmatic framework for the practising clinician.
Keywords: CSF; clinical neurology; headache; neuroradiology; neurosurgery.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources