

Best case/worst case for the trauma ICU: Development and pilot testing of a communication tool for older adults with traumatic injury
- PMID: 34039930
- PMCID: PMC8939782
- DOI: 10.1097/TA.0000000000003281
Best case/worst case for the trauma ICU: Development and pilot testing of a communication tool for older adults with traumatic injury
Abstract
Background: "Best Case/Worst Case" (BC/WC) is a communication tool to support shared decision making in older adults with surgical illness. We aimed to adapt and test BC/WC for use with critically ill older adult trauma patients.
Methods: We conducted focus groups with 48 trauma clinicians in Wisconsin, Texas, and Oregon. We used qualitative content analysis to characterize feedback and adapted the tool to fit this setting. Using rapid sequence iterative design, we developed an implementation tool kit. We pilot tested this intervention at two trauma centers using a pre-post study design with older trauma patients in the intensive care unit (ICU). Main outcome measures included study feasibility, intervention acceptability, quality of communication, and clinician moral distress.
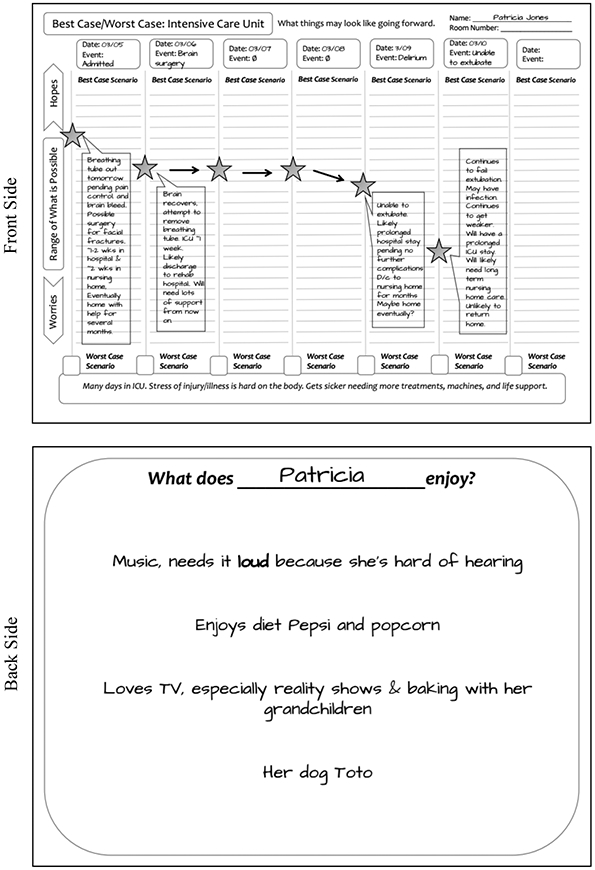
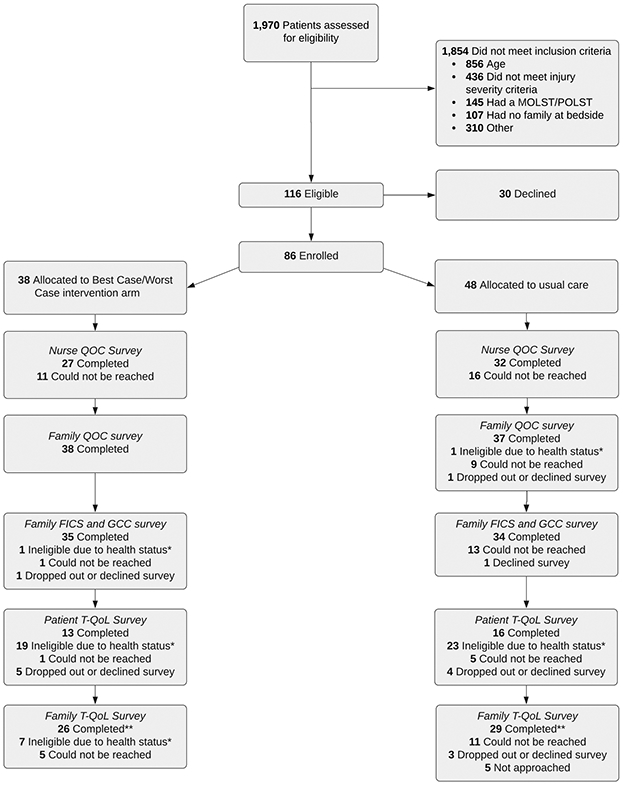
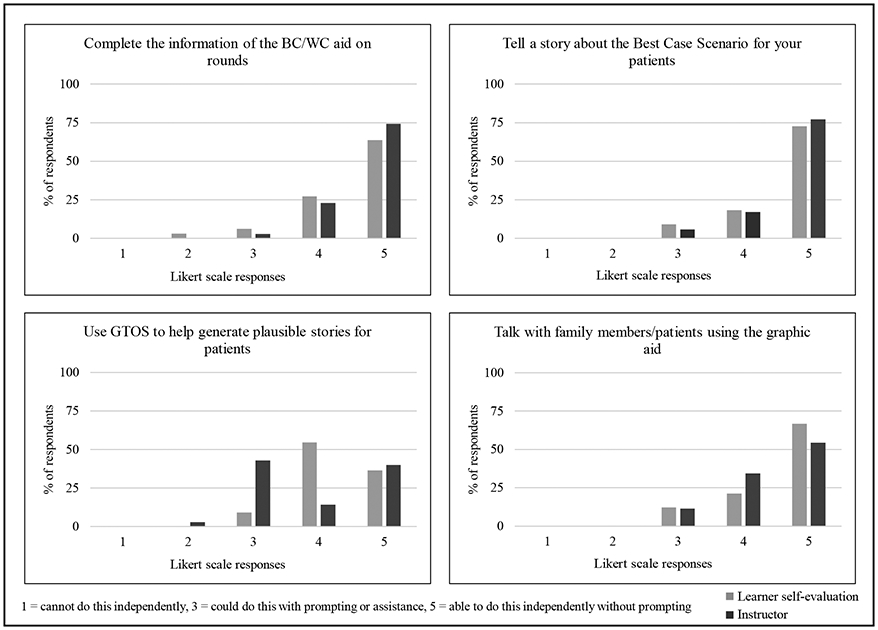
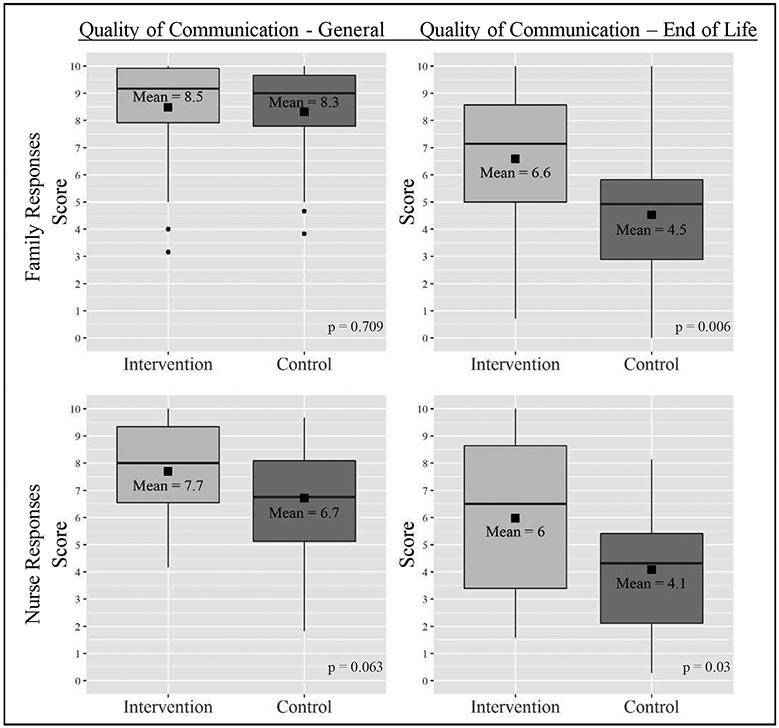
Results: BC/WC for trauma patients uses a graphic aid to document major events over time, illustrate plausible scenarios, and convey uncertainty. We enrolled 86 of 116 eligible patients and their surrogates (48 pre/38 postintervention). The median patient age was 72 years (51-95 years) and mean Geriatric Trauma Outcome Score was 126.1 (±30.6). We trained 43 trauma attendings and trauma fellows to use the intervention. Ninety-four percent could perform essential tool elements after training. The median end-of-life communication score (scale 0-10) improved from 4.5 to 6.6 (p = 0.006) after intervention as reported by family and from 4.1 to 6.0 (p = 0.03) as reported by nurses. Moral distress did not change. However, there was improvement (less distress) reported by physicians regarding "witnessing providers giving false hope" from 7.34 to 5.03 (p = 0.022). Surgeons reported the tool put multiple clinicians on the same page and was useful for families, but tedious to incorporate into rounds.
Conclusion: BC/WC trauma ICU is acceptable to clinicians and may support improved communication in the ICU. Future efficacy testing is threatened by enrollment challenges for severely injured older adults and their family members.
Level of evidence: Therapeutic, level III.
Trial registration: ClinicalTrials.gov NCT03188055.
Copyright © 2021 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
Conflict of Interest Statement:
The authors have no relevant financial conflicts of interest to declare.
Figures
References
-
- National Center for Injury Prevention and Control. 10 Leading Causes of Nonfatal Injuries, United States, 2014, All Races, Both Sexes, Disposition: All Cases, Ages: 65-85 Available from: webappa.cdc.gov/sasweb/ncipc/nfilead2001.html.
-
- Fried TR, Bradley EH, Towle VR, Allore H. Understanding the treatment preferences of seriously ill patients. N Engl J Med. 2002;346(14):1061–6. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
