

Urinary fatty acid binding protein 3 (uFABP3) is a potential biomarker for peripheral arterial disease
- PMID: 34040076
- PMCID: PMC8155078
- DOI: 10.1038/s41598-021-90395-0
Urinary fatty acid binding protein 3 (uFABP3) is a potential biomarker for peripheral arterial disease
Abstract
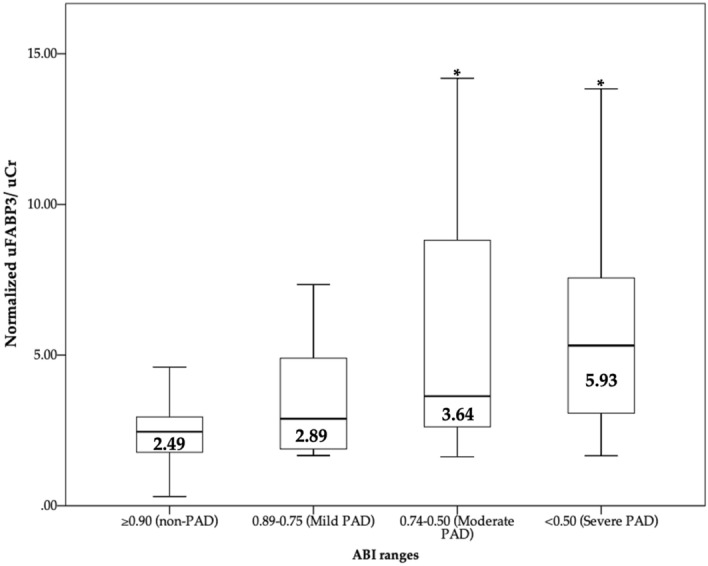
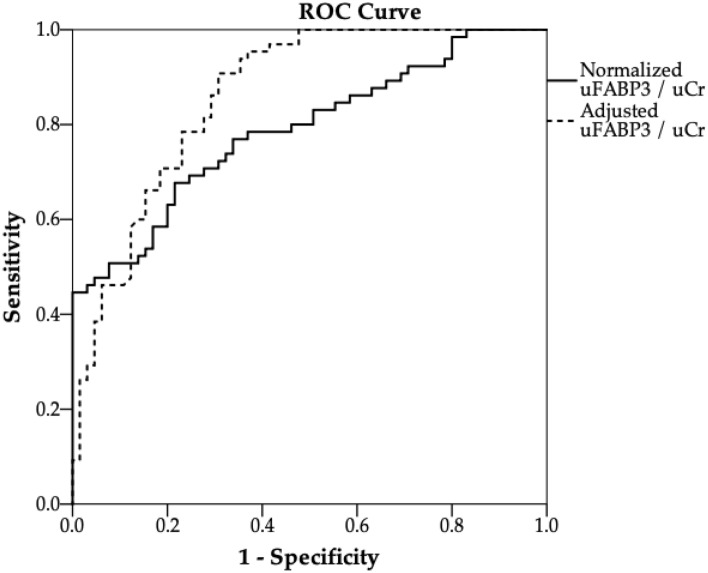
Plasma levels of fatty acid binding protein 3 (pFABP3) are elevated in patients with peripheral artery disease (PAD). Since the kidney filters FABP3 from circulation, we investigated whether urinary fatty acid binding protein 3 (uFABP3) is associated with PAD, and also explored its potential as a diagnostic biomarker for this disease state. A total of 130 patients were recruited from outpatient clinics at St. Michael's Hospital, comprising of 65 patients with PAD and 65 patients without PAD (non-PAD). Levels of uFABP3 normalized for urine creatinine (uFABP3/uCr) were 1.7-folds higher in patients with PAD [median (IQR) 4.41 (2.79-8.08)] compared with non-PAD controls [median (IQR) 2.49 (1.78-3.12), p-value = 0.001]. Subgroup analysis demonstrated no significant effect of cardiovascular risk factors (age, sex, hypertension, hypercholesteremia, diabetes and smoking) on uFABP3/uCr in both PAD and non-PAD patients. Spearmen correlation studies demonstrated a significant negative correlation between uFABP3/uCr and ABI (ρ = - 0.436; p-value = 0.001). Regression analysis demonstrated that uFABP3/Cr levels were associated with PAD independently of age, sex, hypercholesterolemia, smoking, prior history of coronary arterial disease and Estimated Glomerular Filtration rate (eGFR) [odds ratio: 2.34 (95% confidence interval: 1.47-3.75) p-value < 0.001]. Lastly, receiver operator curve (ROC) analysis demonstrated unadjusted area under the curve (AUC) for uFABP3/Cr of 0.79, which improved to 0.86 after adjusting for eGFR, age, hypercholesteremia, smoking and diabetes. In conclusion, our results demonstrate a strong association between uFABP3/Cr and PAD and suggest the potential of uFABP3/Cr in identifying patients with PAD.
Conflict of interest statement
Dr. John Eikelboom reports consulting fees/honoraria and/or grant support from Astra-Zeneca, Bayer Boehringer-Ingelheim, Bristol-Myer-Squibb/Pfizer, Daiichi-Sankyo, Eli-Lilly, Glaxo-Smith-Kline, Pfizer, Janssen, Sanofi-Aventis, Servier. The funders also had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results. All other authors declare no competing interests.
Figures
Similar articles
-
Validating fatty acid binding protein 3 as a diagnostic and prognostic biomarker for peripheral arterial disease: A three-year prospective follow-up study.EClinicalMedicine. 2022 Dec 13;55:101766. doi: 10.1016/j.eclinm.2022.101766. eCollection 2023 Jan. EClinicalMedicine. 2022. PMID: 36531981 Free PMC article.
-
Urinary Fatty Acid Binding Protein 3 Has Prognostic Value in Peripheral Artery Disease.Front Cardiovasc Med. 2022 Jun 20;9:875244. doi: 10.3389/fcvm.2022.875244. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35795372 Free PMC article.
-
Elevated plasma levels of NT-proBNP in ambulatory patients with peripheral arterial disease.PLoS One. 2021 Jul 21;16(7):e0253792. doi: 10.1371/journal.pone.0253792. eCollection 2021. PLoS One. 2021. PMID: 34288948 Free PMC article.
-
Fatty acid binding protein 3 is associated with peripheral arterial disease.JVS Vasc Sci. 2020 Sep 2;1:168-175. doi: 10.1016/j.jvssci.2020.08.003. eCollection 2020. JVS Vasc Sci. 2020. PMID: 34617045 Free PMC article.
-
Fatty Acid Binding Protein 4-A Circulating Protein Associated with Peripheral Arterial Disease in Diabetic Patients.J Clin Med. 2020 Sep 2;9(9):2843. doi: 10.3390/jcm9092843. J Clin Med. 2020. PMID: 32887447 Free PMC article.
Cited by
-
The prognostic capability of inflammatory proteins in predicting peripheral artery disease related adverse events.Front Cardiovasc Med. 2022 Dec 13;9:1073751. doi: 10.3389/fcvm.2022.1073751. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36582735 Free PMC article.
-
Identification and Evaluation of Angiogenesis-Related Proteins That Predict Major Adverse Cardiovascular Events in Patients with Peripheral Artery Disease.J Cardiovasc Dev Dis. 2024 Dec 13;11(12):402. doi: 10.3390/jcdd11120402. J Cardiovasc Dev Dis. 2024. PMID: 39728292 Free PMC article.
-
Prediction of Major Adverse Limb Events in Females with Peripheral Artery Disease using Blood-Based Biomarkers and Clinical Features.J Cardiovasc Transl Res. 2025 Apr;18(2):316-330. doi: 10.1007/s12265-024-10574-y. Epub 2024 Dec 6. J Cardiovasc Transl Res. 2025. PMID: 39643751
-
Validating fatty acid binding protein 3 as a diagnostic and prognostic biomarker for peripheral arterial disease: A three-year prospective follow-up study.EClinicalMedicine. 2022 Dec 13;55:101766. doi: 10.1016/j.eclinm.2022.101766. eCollection 2023 Jan. EClinicalMedicine. 2022. PMID: 36531981 Free PMC article.
-
Urinary neutrophil gelatinase-associated lipocalin (NGAL) can potentially predict vascular complications and reliably risk stratify patients with peripheral arterial disease.Sci Rep. 2022 May 18;12(1):8312. doi: 10.1038/s41598-022-12286-2. Sci Rep. 2022. PMID: 35585171 Free PMC article.
References
-
- Sampson, U. K. et al. Global and regional burden of death and disability from peripheral artery disease: 21 world regions, 1990 to 2010. Global Heart9, 145–158.e121 (2014). - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
