

The risk of contralateral breast cancer: a SEER-based analysis
- PMID: 34040177
- PMCID: PMC8368197
- DOI: 10.1038/s41416-021-01417-7
The risk of contralateral breast cancer: a SEER-based analysis
Abstract
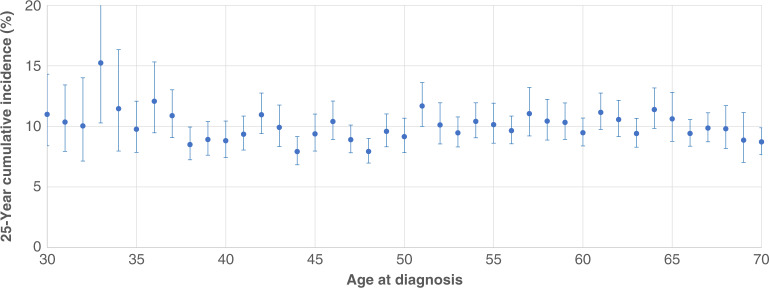
Background: We sought to estimate the annual risk and 25-year cumulative risk of contralateral breast cancer among women with stage 0-III unilateral breast cancer.
Methods: We identified 812,851 women with unilateral breast cancer diagnosed between 1990 and 2015 in the SEER database and followed them for contralateral breast cancer for up to 25 years. Women with a known bilateral mastectomy were excluded. We calculated the annual risk of contralateral breast cancer by age at diagnosis, by time since diagnosis and by current age. We compared risks by ductal carcinoma in situ (DCIS) versus invasive disease, by race and by oestrogen receptor (ER) status of the first cancer.
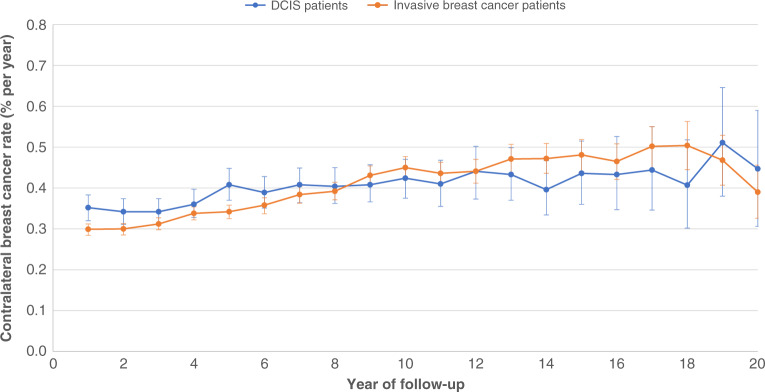
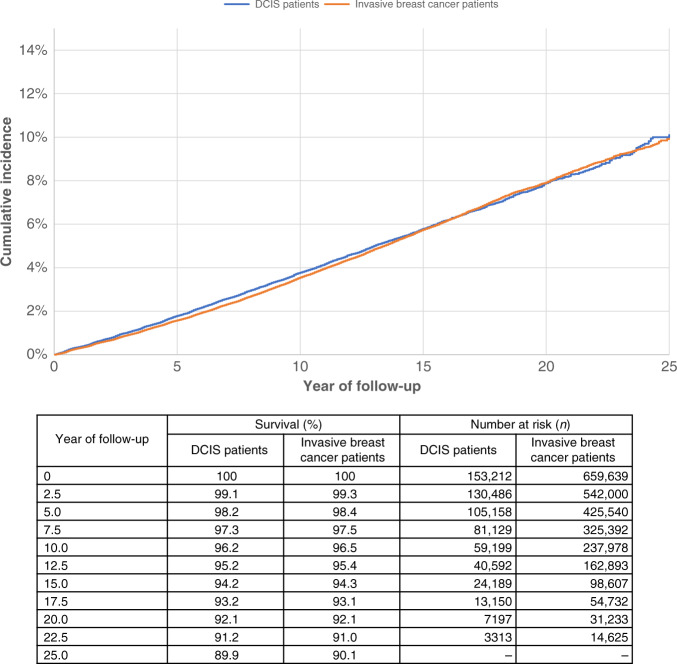
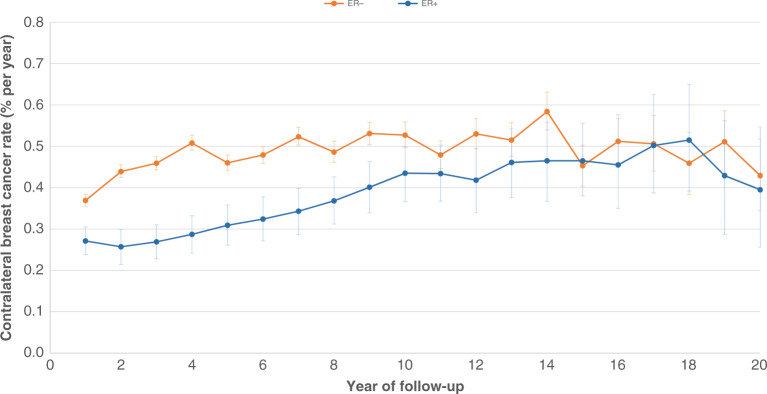
Results: There were 25,958 cases of contralateral invasive breast cancer diagnosed (3.2% of all patients). The annual risk of contralateral breast cancer over the 25-year follow-up period was 0.37% and the 25-year actuarial risk of contralateral invasive breast cancer was 9.9%. The annual risk varied to a small degree by age of diagnosis, by time elapsed since diagnosis and by current age. The 25-year actuarial risk was similar for DCIS and invasive breast cancer patients (10.1 versus 9.9%). The 25-year actuarial risk was higher for black women (12.7%) than for white women (9.7%) and was lower for women with ER-positive breast cancer (9.5%) than for women with ER-negative breast cancer (11.2%).
Conclusions: Women with unilateral breast cancer experience an annual risk of contralateral breast cancer ~0.4% per year, which persists over the 25-year follow-up period.
© 2021. The Author(s), under exclusive licence to Springer Nature Limited.
Conflict of interest statement
S.A.N. is an editorial board member of BJC. All other authors declare no competing interests.
Figures
References
-
- Nash R, Goodman M, Lin CC, Freedman RA, Dominici LS, Ward K, et al. State variation in the receipt of a contralateral prophylactic mastectomy among women who received a diagnosis of invasive unilateral early-stage breast cancer in the United States, 2004-2012. JAMA Surg. 2017;152:648–657. doi: 10.1001/jamasurg.2017.0115. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
