

Electrodiagnostic, Sonographic, and Clinical Features of Carpal Tunnel Syndrome with Bifid Median Nerve
- PMID: 34040430
- PMCID: PMC8140939
- DOI: 10.2147/JPR.S303142
Electrodiagnostic, Sonographic, and Clinical Features of Carpal Tunnel Syndrome with Bifid Median Nerve
Abstract
Purpose: A bifid median nerve (BMN) is not a rare variant. This study aimed to investigate the features of carpal tunnel syndrome (CTS) accompanied by BMN.
Patients and methods: In this retrospective study, we defined a BMN group as CTS with BMN and a non-bifid median nerve (NMN) group as CTS without BMN. All hands were assigned to four severity grades according to the findings of electrodiagnosis (EDx): very mild, mild, moderate, and severe. The cross-sectional area (CSA) of the median nerve, palmar bowing of the flexor retinaculum, and persistent median artery (PMA) were assessed by ultrasonography. Numerical pain rating scale (NRS) and symptom duration were assessed as clinical variables.
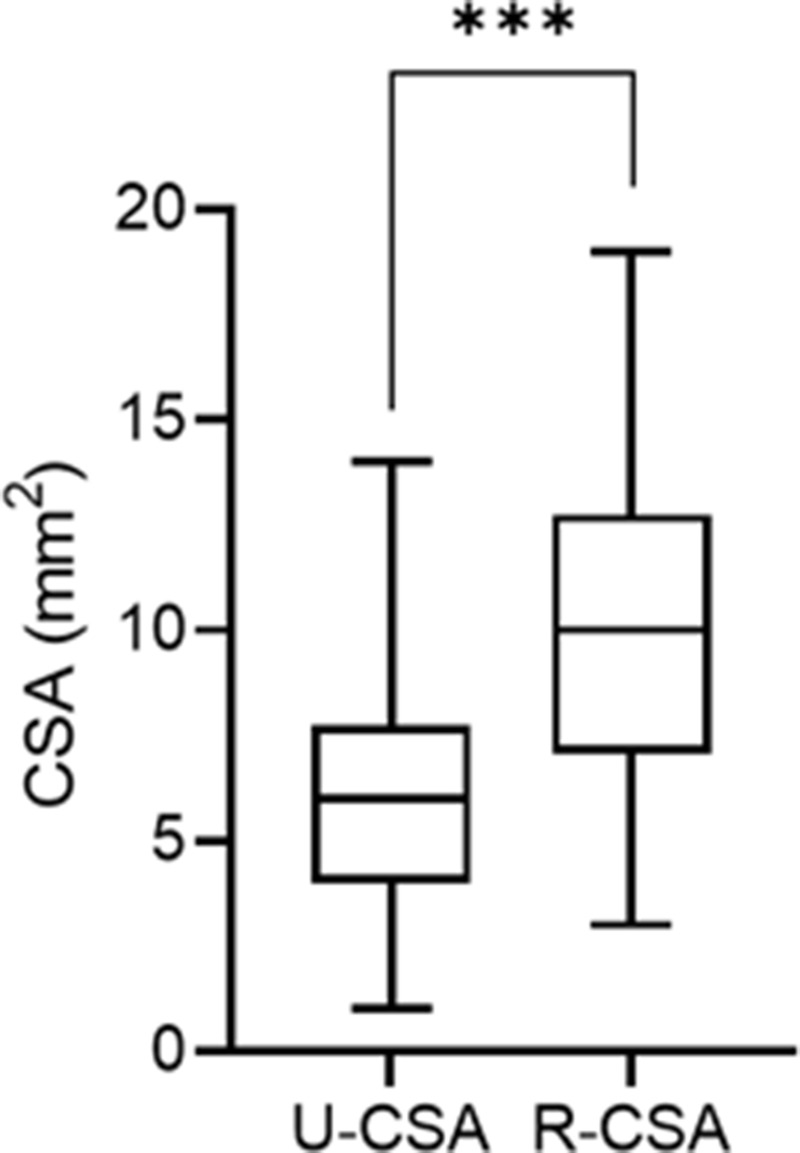
Results: Sixty-four hands (57 patients) and 442 hands (341 patients) were enrolled in the BMN and the NMN groups, respectively. BMN was prevalent in 12.6% of all CTS hands. The distribution of EDx severity grade was milder in the BMN group than in the NMN group (P<0.001). The CSA of the BMN group was 16.2±4.1 mm2, slightly larger than 15.1±4.2 mm2 in the NMN group (P=0.056). The BMN group showed higher NRS than the NMN group (5.5±1.5 and 4.4±1.7, respectively; P<0.001). In the subgroup analysis, NRS was significantly higher in the BMN group than in the NMN group at all EDx severity grades. In the BMN group, the PMA group showed greater EDx severity (P=0.037) and higher NRS (6.0 and 5.0, respectively; P=0.012) than the non-PMA group. The radial side branch's CSA was larger than that of the ulnar side branch (10.0 mm2 and 6.0 mm2, respectively; P<0.001).
Conclusion: CTS with BMN presented more severe symptoms and relatively milder EDx severity. When assessing the severity of CTS with BMN, the clinical symptoms should primarily be considered, as well as we should complementarily evaluate the EDx and ultrasonography.
Keywords: bifid median nerve; carpal tunnel syndrome; diagnostic ultrasound; electrodiagnosis; pain measurement.
© 2021 Park et al.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures




Similar articles
-
Median Nerve Cross-Sectional Area and Carpal Tunnel Syndrome in Specific Populations: Sonographic Analysis of Patients With Type 2 Diabetes or Bifid Anatomy.J Ultrasound Med. 2024 Sep;43(9):1683-1694. doi: 10.1002/jum.16491. Epub 2024 May 30. J Ultrasound Med. 2024. PMID: 38813705
-
Severity of Carpal tunnel syndrome assessed with high frequency ultrasonography.Rheumatol Int. 2010 Apr;30(6):761-5. doi: 10.1007/s00296-009-1061-x. Epub 2009 Jul 11. Rheumatol Int. 2010. PMID: 19593567
-
Correlation between Ultrasonography Findings and Electrodiagnostic Severity in Carpal Tunnel Syndrome: 3D Ultrasonography.J Clin Neurol. 2014 Oct;10(4):348-53. doi: 10.3988/jcn.2014.10.4.348. Epub 2014 Oct 6. J Clin Neurol. 2014. PMID: 25324885 Free PMC article.
-
Expert consensus on the combined investigation of carpal tunnel syndrome with electrodiagnostic tests and neuromuscular ultrasound.Clin Neurophysiol. 2022 Mar;135:107-116. doi: 10.1016/j.clinph.2021.12.012. Epub 2022 Jan 6. Clin Neurophysiol. 2022. PMID: 35074720 Review.
-
Hand surgeons and amyloidosis specialists warning: transthyretin-associated amyloidosis with bifid median nerve as a cause of bilateral carpal tunnel syndrome. A case report and literature review.Eur J Orthop Surg Traumatol. 2022 Apr;32(3):575-581. doi: 10.1007/s00590-021-03004-1. Epub 2021 May 29. Eur J Orthop Surg Traumatol. 2022. PMID: 34050818 Review.
Cited by
-
Application of digital infrared thermography for carpal tunnel syndrome evaluation.Sci Rep. 2021 Nov 9;11(1):21963. doi: 10.1038/s41598-021-01381-5. Sci Rep. 2021. PMID: 34754001 Free PMC article.
-
Coexistence of anomalous muscle, persistent median artery, bifid median nerve causing carpal tunnel syndrome: A case report and literature review.Front Pediatr. 2023 Feb 9;11:1043442. doi: 10.3389/fped.2023.1043442. eCollection 2023. Front Pediatr. 2023. PMID: 36846165 Free PMC article.
-
Characteristics of diabetic and non-diabetic carpal tunnel syndrome in terms of clinical, electrophysiological, and Sonographic features: a cross-sectional study.BMC Musculoskelet Disord. 2023 Sep 16;24(1):739. doi: 10.1186/s12891-023-06881-1. BMC Musculoskelet Disord. 2023. PMID: 37716949 Free PMC article.
-
Anatomical variations and their association with carpal tunnel syndrome: a comparison with healthy controls.Int Orthop. 2025 Apr;49(4):911-917. doi: 10.1007/s00264-025-06480-w. Epub 2025 Mar 13. Int Orthop. 2025. PMID: 40080129
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
