

Global Burden of Aortic Aneurysm and Attributable Risk Factors from 1990 to 2017
- PMID: 34040948
- PMCID: PMC8103850
- DOI: 10.5334/gh.920
Global Burden of Aortic Aneurysm and Attributable Risk Factors from 1990 to 2017
Abstract
Background: To date, our understanding of the global aortic aneurysm (AA) burden distribution is very limited.
Objective: To assess a full view of global AA burden distribution and attributable risk factors from 1990 to 2017.
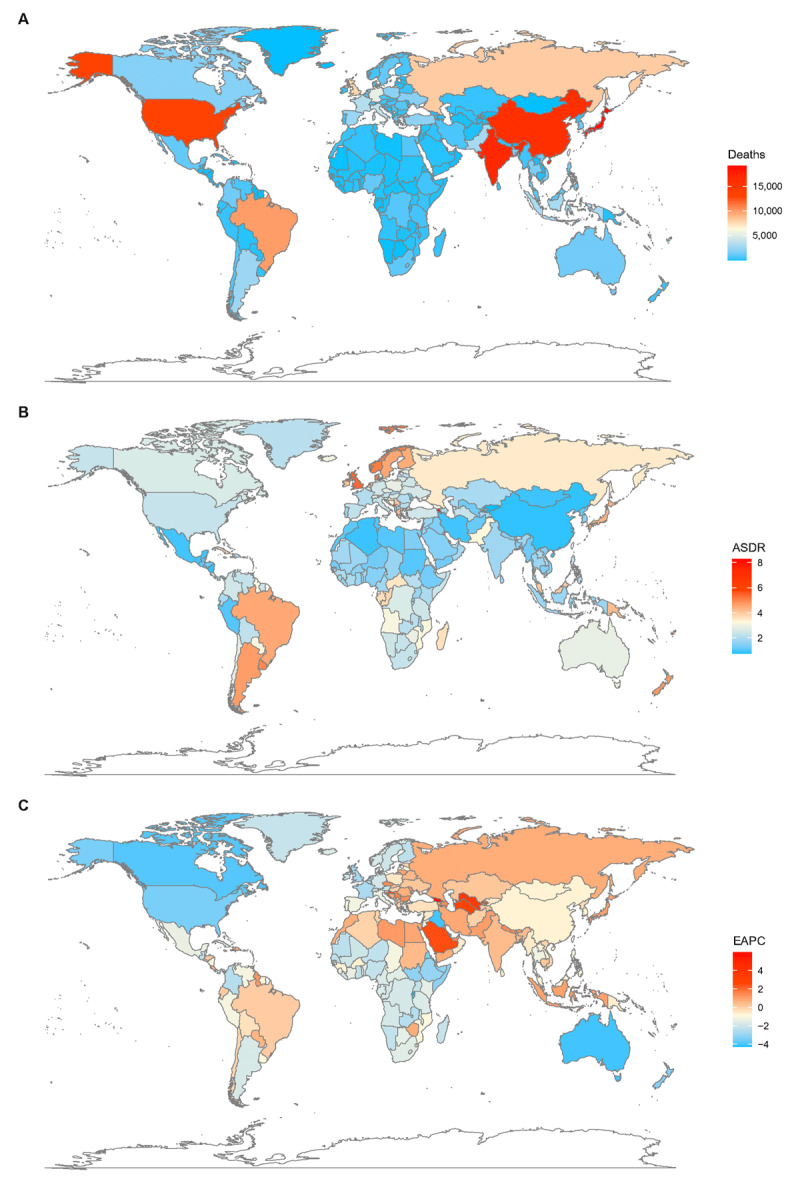
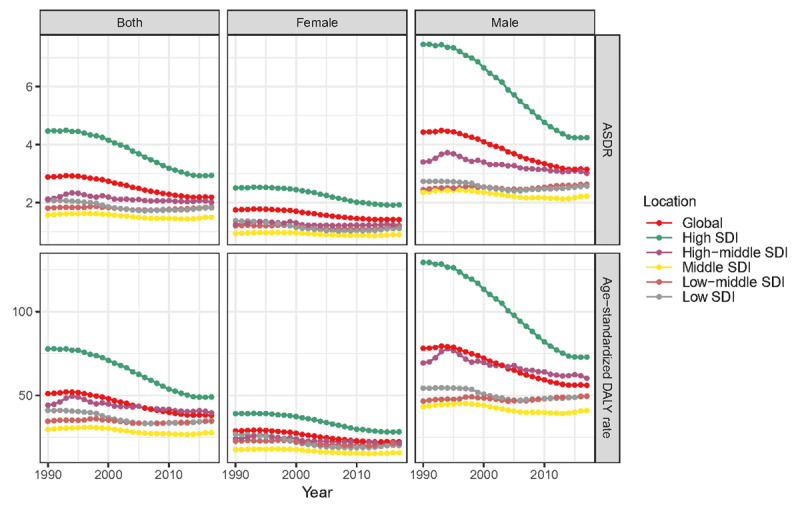
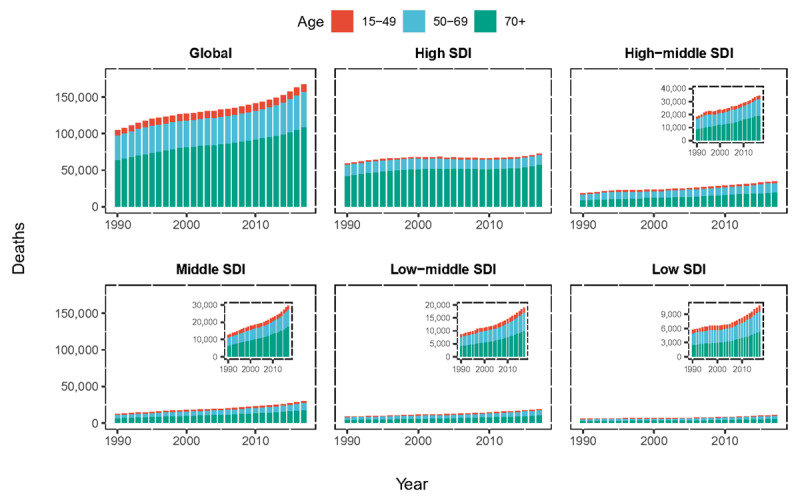
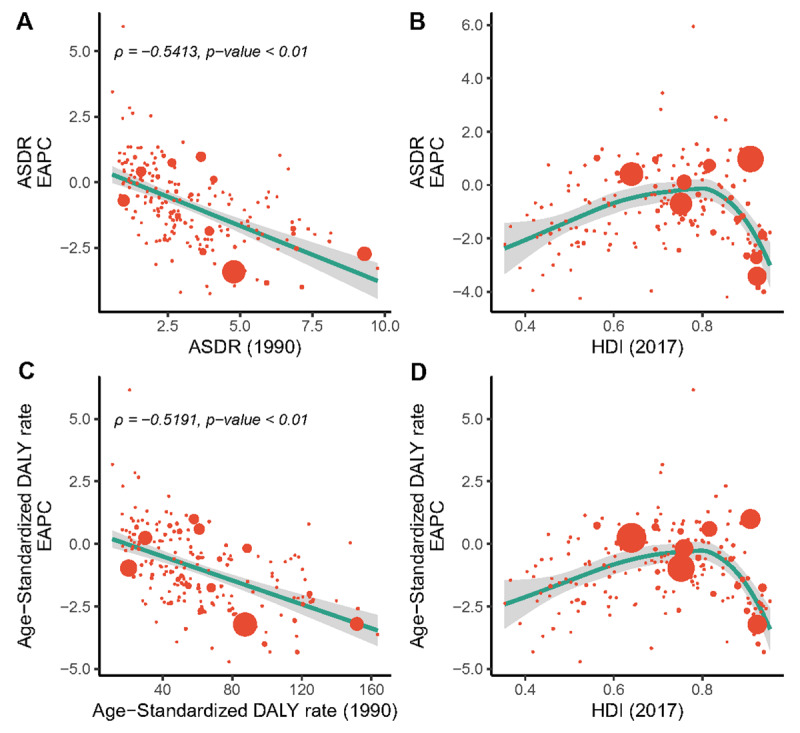
Methods: We extracted data of AA deaths, disability-adjusted life years (DALYs), and their corresponding age-standardized rates (ASRs), in general and by age/sex from the 2017 Global Burden of Disease (GBD) study. The current AA burden distribution in 2017 and its changing trend from 1990 to 2017 were separately showed. The spatial divergence was discussed from four levels: global, five social-demographic index regions, 21 GBD regions, and 195 countries and territories. We also estimated the risk factors attributable to AA related deaths.
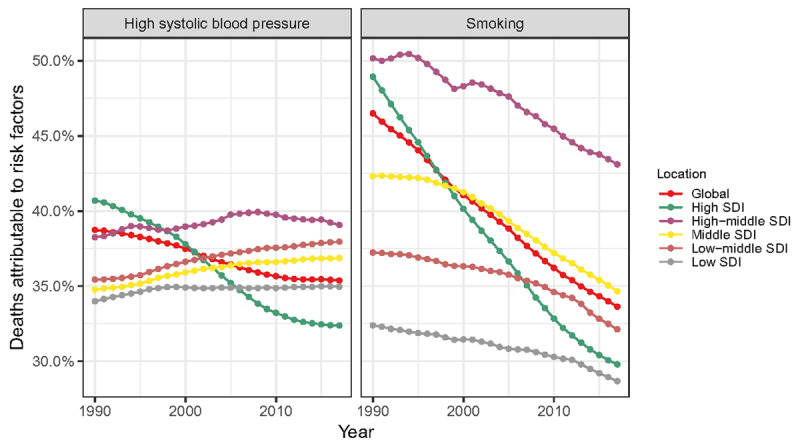
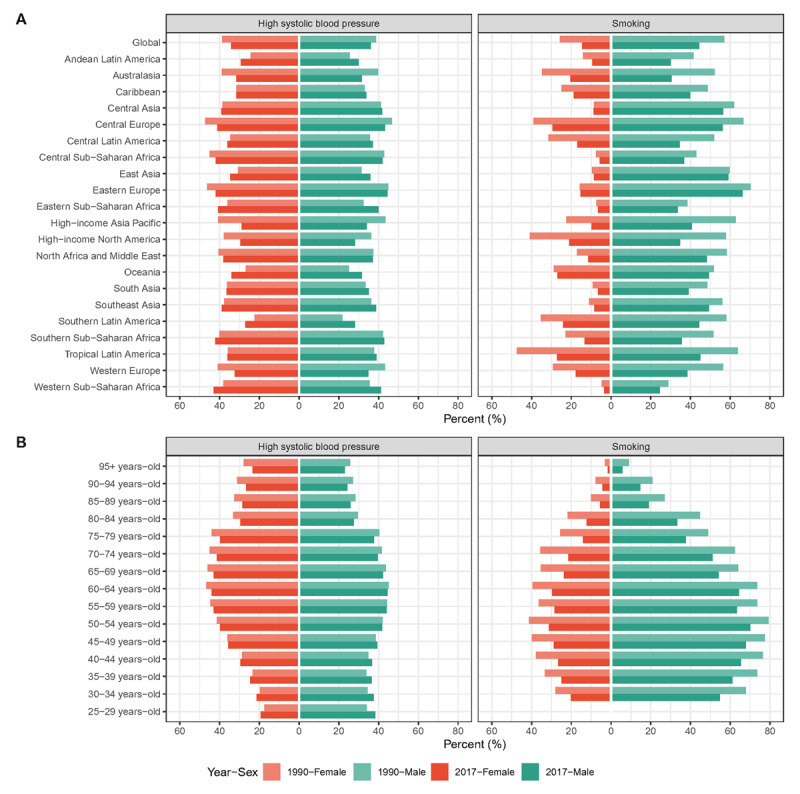
Results: Globally, the AA deaths were 167,249 with an age-standardized death rate (ASDR) of 2.19/100,000 persons in 2017, among which the elderly and the males accounted for the majority. Although reductions in ASRs were observed in developed areas, AA remained an important health issue in those relatively underdeveloped areas and might be much more important in the near future. AA may increasingly affect the elderly and the female population. Similar patterns of AA DALYs burden were noted during the study period. AA burden attributable to high blood pressure and smoking decreased globally and there were many heterogeneities in their distribution.
Discussion: AA maintained an incremental public health issue worldwide. The change pattern of AA burden was heterogeneous across locations, ages, and sexes and it is paramount to improve resource allocation for more effective and targeted prevention strategies. Also, prevention of tobacco consumption and blood pressure control should be emphasized.
Keywords: aortic aneurysm; deaths; disability-adjusted life years; global burden of disease; risk factors.
Copyright: © 2021 The Author(s).
Conflict of interest statement
The authors have no competing interests to declare.
Figures
References
-
- Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet (London, England). 2018; 392(10159): 1859–922. DOI: 10.1016/S0140-6736(18)32335-3 - DOI - PMC - PubMed
-
- Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet (London, England). 2018; 392(10159): 1923–94. DOI: 10.1016/S0140-6736(18)32225-6 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
