

Making a Cold Tumor Hot: The Role of Vaccines in the Treatment of Glioblastoma
- PMID: 34041034
- PMCID: PMC8141615
- DOI: 10.3389/fonc.2021.672508
Making a Cold Tumor Hot: The Role of Vaccines in the Treatment of Glioblastoma
Abstract
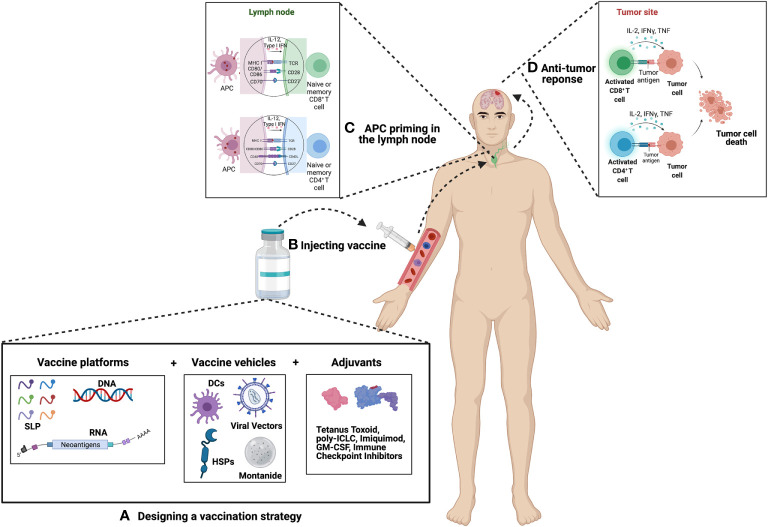
The use of immunotherapies for the treatment of brain tumors is a topic that has garnered considerable excitement in recent years. Discoveries such as the presence of a glymphatic system and immune surveillance in the central nervous system (CNS) have shattered the theory of immune privilege and opened up the possibility of treating CNS malignancies with immunotherapies. However, despite many immunotherapy clinical trials aimed at treating glioblastoma (GBM), very few have demonstrated a significant survival benefit. Several factors for this have been identified, one of which is that GBMs are immunologically "cold," implying that the cancer does not induce a strong T cell response. It is postulated that this is why clinical trials using an immune checkpoint inhibitor alone have not demonstrated efficacy. While it is well established that anti-cancer T cell responses can be facilitated by the presentation of tumor-specific antigens to the immune system, treatment-related death of GBM cells and subsequent release of molecules have not been shown to be sufficient to evoke an anti-tumor immune response effective enough to have a significant impact. To overcome this limitation, vaccines can be used to introduce exogenous antigens at higher concentrations to the immune system to induce strong tumor antigen-specific T cell responses. In this review, we will describe vaccination strategies that are under investigation to treat GBM; categorizing them based on their target antigens, form of antigens, vehicles used, and pairing with specific adjuvants. We will review the concept of vaccine therapy in combination with immune checkpoint inhibitors, as it is hypothesized that this approach may be more effective in overcoming the immunosuppressive milieu of GBM. Clinical trial design and the need for incorporating robust immune monitoring into future studies will also be discussed here. We believe that the integration of evolving technologies of vaccine development, delivery, and immune monitoring will further enhance the role of these therapies and will likely remain an important area of investigation for future treatment strategies for GBM patients.
Keywords: T cells; dendritic cells; glioblastoma; heat shock protein; neoantigen; peptide; tumor antigen; vaccine.
Copyright © 2021 Frederico, Hancock, Brettschneider, Ratnam, Gilbert and Terabe.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Immunotherapy as a New Therapeutic Approach for Brain and Spinal Cord Tumors.Adv Exp Med Biol. 2023;1394:73-84. doi: 10.1007/978-3-031-14732-6_5. Adv Exp Med Biol. 2023. PMID: 36587382
-
Emerging immunotherapies for glioblastoma.Expert Opin Emerg Drugs. 2016 Jun;21(2):133-45. doi: 10.1080/14728214.2016.1186643. Expert Opin Emerg Drugs. 2016. PMID: 27223671 Free PMC article. Review.
-
Combinatorial approaches to effective therapy in glioblastoma (GBM): Current status and what the future holds.Int Rev Immunol. 2022;41(6):582-605. doi: 10.1080/08830185.2022.2101647. Epub 2022 Aug 8. Int Rev Immunol. 2022. PMID: 35938932 Review.
-
Translational landscape of glioblastoma immunotherapy for physicians: guiding clinical practice with basic scientific evidence.J Hematol Oncol. 2022 Jun 11;15(1):80. doi: 10.1186/s13045-022-01298-0. J Hematol Oncol. 2022. PMID: 35690784 Free PMC article. Review.
-
Neoadjuvant immune checkpoint inhibition in the management of glioblastoma: Exploring a new frontier.Front Immunol. 2023 Feb 17;14:1057567. doi: 10.3389/fimmu.2023.1057567. eCollection 2023. Front Immunol. 2023. PMID: 36875096 Free PMC article. Review.
Cited by
-
Current Status and Challenges of Vaccination Therapy for Glioblastoma.Mol Cancer Ther. 2023 Apr 3;22(4):435-446. doi: 10.1158/1535-7163.MCT-22-0503. Mol Cancer Ther. 2023. PMID: 36779991 Free PMC article.
-
Polyclonal antibody-induced downregulation of HER1/EGFR and HER2 surpasses the effect of combinations of specific registered antibodies.Front Oncol. 2022 Nov 2;12:951267. doi: 10.3389/fonc.2022.951267. eCollection 2022. Front Oncol. 2022. PMID: 36408164 Free PMC article.
-
An update on the molecular biology of glioblastoma, with clinical implications and progress in its treatment.Cancer Commun (Lond). 2022 Nov;42(11):1083-1111. doi: 10.1002/cac2.12361. Epub 2022 Sep 21. Cancer Commun (Lond). 2022. PMID: 36129048 Free PMC article. Review.
-
CAR-T Therapy in GBM: Current Challenges and Avenues for Improvement.Cancers (Basel). 2023 Feb 16;15(4):1249. doi: 10.3390/cancers15041249. Cancers (Basel). 2023. PMID: 36831591 Free PMC article. Review.
-
Myeloid cells as potential targets for immunotherapy in pediatric gliomas.Front Pediatr. 2024 Mar 8;12:1346493. doi: 10.3389/fped.2024.1346493. eCollection 2024. Front Pediatr. 2024. PMID: 38523840 Free PMC article. Review.
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources