

Resuscitation in Paediatric Sepsis Using Metabolic Resuscitation-A Randomized Controlled Pilot Study in the Paediatric Intensive Care Unit (RESPOND PICU): Study Protocol and Analysis Plan
- PMID: 34041208
- PMCID: PMC8142861
- DOI: 10.3389/fped.2021.663435
Resuscitation in Paediatric Sepsis Using Metabolic Resuscitation-A Randomized Controlled Pilot Study in the Paediatric Intensive Care Unit (RESPOND PICU): Study Protocol and Analysis Plan
Abstract
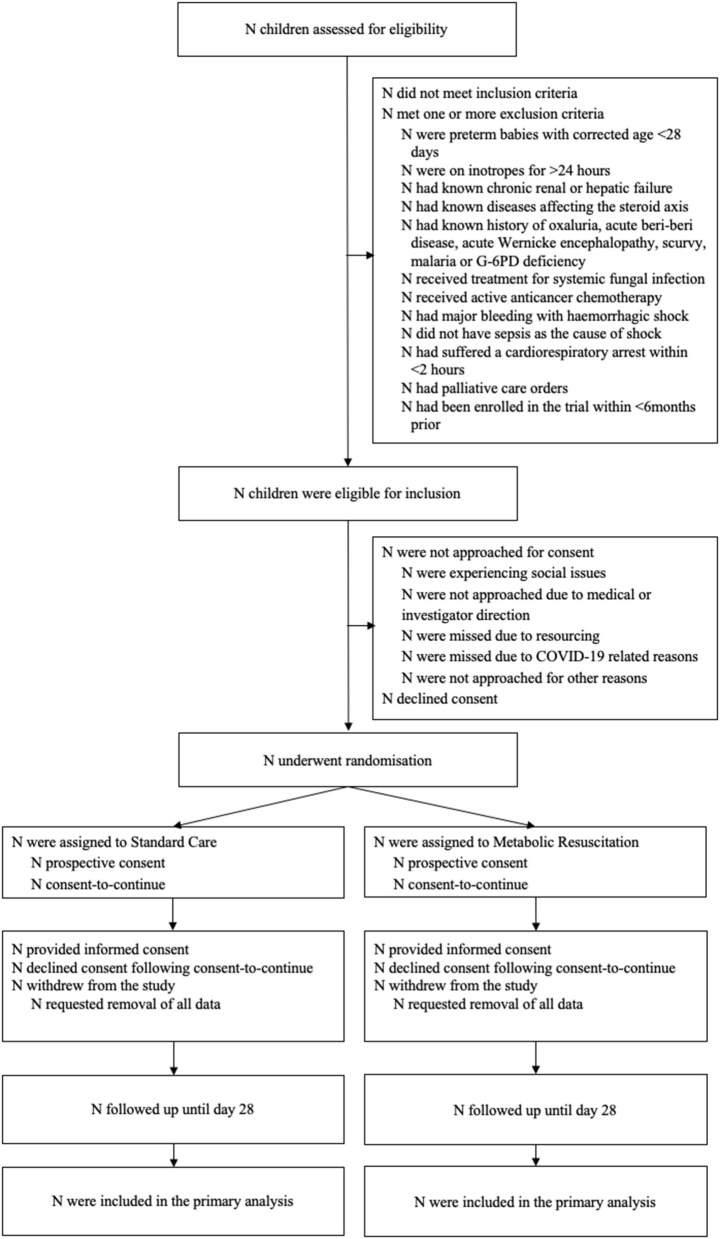
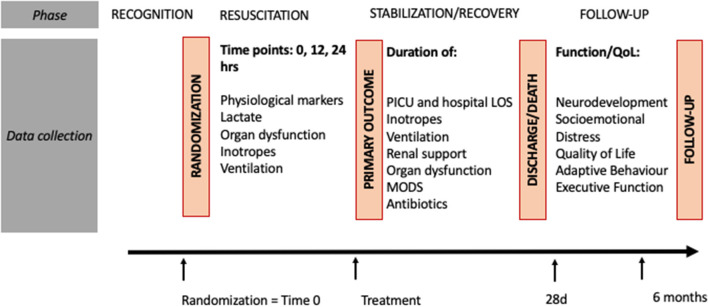
Introduction: Septic shock remains amongst the leading causes of childhood mortality. Therapeutic options to support children with septic shock refractory to initial resuscitation with fluids and inotropes are limited. Recently, the combination of intravenous hydrocortisone with high dose ascorbic acid and thiamine (HAT therapy), postulated to reduce sepsis-related organ dysfunction, has been proposed as a safe approach with potential for mortality benefit, but randomized trials in paediatric patients are lacking. We hypothesize that protocolised early use of HAT therapy ("metabolic resuscitation") in children with septic shock is feasible and will lead to earlier resolution of organ dysfunction. Here, we describe the protocol of the Resuscitation in Paediatric Sepsis Using Metabolic Resuscitation-A Randomized Controlled Pilot Study in the Paediatric Intensive Care Unit (RESPOND PICU). Methods and Analysis: The RESPOND PICU study is an open label randomized-controlled, two-sided multicentre pilot study conducted in paediatric intensive care units (PICUs) in Australia and New Zealand. Sixty children aged between 28 days and 18 years treated with inotropes for presumed septic shock will be randomized in a 1:1 ratio to either metabolic resuscitation (1 mg/kg hydrocortisone q6h, 30 mg/kg ascorbic acid q6h, 4 mg/kg thiamine q12h) or standard septic shock management. Main outcomes include feasibility of the study protocol and survival free of organ dysfunction censored at 28 days. The study cohort will be followed up at 28-days and 6-months post enrolment to assess neurodevelopment, quality of life and functional status. Biobanking will allow ancillary studies on sepsis biomarkers. Ethics and Dissemination: The study received ethical clearance from Children's Health Queensland Human Research Ethics Committee (HREC/18/QCHQ/49168) and commenced enrolment on June 12th, 2019. The primary study findings will be submitted for publication in a peer-reviewed journal. Trial Registration: Australian and New Zealand Clinical Trials Registry (ACTRN12619000829112). Protocol Version: V1.8 22/7/20.
Keywords: ascorbic acid; child; hydrocortisone; intensive care; sepsis; septic shock; thiamine; vitamin C.
Copyright © 2021 Schlapbach, Gibbons, Ridolfi, Harley, Cree, Long, Buckley, Erickson, Festa, George, King, Singh, Raman, Bellomo and the RESPOND PICU study investigators and the Australian New Zealand Intensive Care Society Paediatric Study Group (ANZICS PSG).
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Early Resuscitation in Paediatric Sepsis Using Inotropes - A Randomised Controlled Pilot Study in the Emergency Department (RESPOND ED): Study Protocol and Analysis Plan.Front Pediatr. 2021 May 31;9:663028. doi: 10.3389/fped.2021.663028. eCollection 2021. Front Pediatr. 2021. PMID: 34136441 Free PMC article.
-
Resuscitation With Vitamin C, Hydrocortisone, and Thiamin in Children With Septic Shock: A Multicenter Randomized Pilot Study.Pediatr Crit Care Med. 2024 Feb 1;25(2):159-170. doi: 10.1097/PCC.0000000000003346. Epub 2024 Jan 19. Pediatr Crit Care Med. 2024. PMID: 38240537 Free PMC article. Clinical Trial.
-
Resuscitation in Paediatric Septic Shock Using Vitamin C and Hydrocortisone (RESPOND): The RESPOND Randomized Controlled Trial Protocol.Pediatr Crit Care Med. 2025 Mar 1;26(3):e374-e385. doi: 10.1097/PCC.0000000000003674. Epub 2024 Dec 26. Pediatr Crit Care Med. 2025. PMID: 39724024 Free PMC article.
-
Metabolic resuscitation in pediatric sepsis: a narrative review.Transl Pediatr. 2021 Oct;10(10):2678-2688. doi: 10.21037/tp-21-1. Transl Pediatr. 2021. PMID: 34765493 Free PMC article. Review.
-
Benefits of combination therapy of hydrocortisone, ascorbic acid and thiamine in sepsis and septic shock: A systematic review.Nutr Health. 2022 Mar;28(1):77-93. doi: 10.1177/02601060211018371. Epub 2021 May 26. Nutr Health. 2022. PMID: 34039089
Cited by
-
Longitudinal cohort study investigating neurodevelopmental and socioemotional outcomes in school-entry aged children after open heart surgery in Australia and New Zealand: the NITRIC follow-up study protocol.BMJ Open. 2023 Aug 30;13(8):e075429. doi: 10.1136/bmjopen-2023-075429. BMJ Open. 2023. PMID: 37648380 Free PMC article.
-
Early Resuscitation in Paediatric Sepsis Using Inotropes - A Randomised Controlled Pilot Study in the Emergency Department (RESPOND ED): Study Protocol and Analysis Plan.Front Pediatr. 2021 May 31;9:663028. doi: 10.3389/fped.2021.663028. eCollection 2021. Front Pediatr. 2021. PMID: 34136441 Free PMC article.
-
Resuscitation With Vitamin C, Hydrocortisone, and Thiamin in Children With Septic Shock: A Multicenter Randomized Pilot Study.Pediatr Crit Care Med. 2024 Feb 1;25(2):159-170. doi: 10.1097/PCC.0000000000003346. Epub 2024 Jan 19. Pediatr Crit Care Med. 2024. PMID: 38240537 Free PMC article. Clinical Trial.
-
The Australian and New Zealand Intensive Care Society Paediatric Study Group (ANZICS PSG): 20 Years of Collaborative Research.Pediatr Crit Care Med. 2025 Jan 1;26(1):e122-e130. doi: 10.1097/PCC.0000000000003653. Epub 2024 Dec 17. Pediatr Crit Care Med. 2025. PMID: 39688453 Free PMC article. No abstract available.
-
Resuscitation in Paediatric Septic Shock Using Vitamin C and Hydrocortisone (RESPOND): The RESPOND Randomized Controlled Trial Protocol.Pediatr Crit Care Med. 2025 Mar 1;26(3):e374-e385. doi: 10.1097/PCC.0000000000003674. Epub 2024 Dec 26. Pediatr Crit Care Med. 2025. PMID: 39724024 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical