

Estimating the effect of nutritional interventions using observational data: the American Heart Association's 2020 Dietary Goals and mortality
- PMID: 34041538
- PMCID: PMC8326054
- DOI: 10.1093/ajcn/nqab100
Estimating the effect of nutritional interventions using observational data: the American Heart Association's 2020 Dietary Goals and mortality
Abstract
Background: Because randomized trials of sustained dietary changes are sometimes impractical for long-term outcomes, the explicit emulation of a (hypothetical) target trial using observational data may be an important tool for nutritional epidemiology.
Objectives: We describe a methodological approach that aims to emulate a target trial of dietary interventions sustained over many years using data from observational cohort studies.
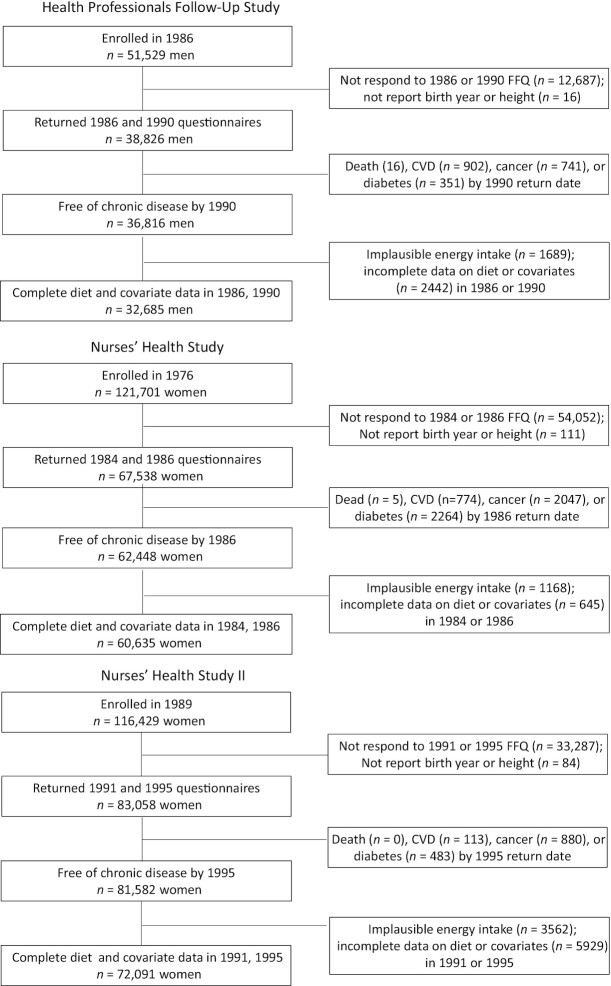
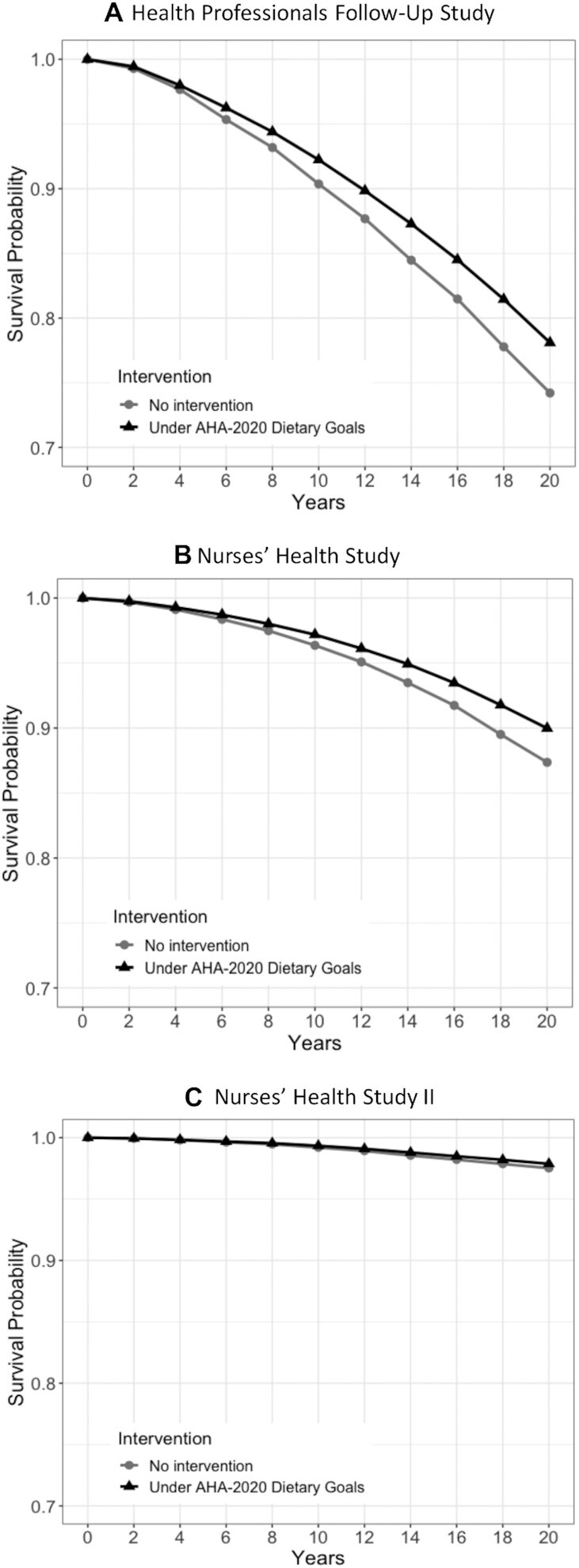
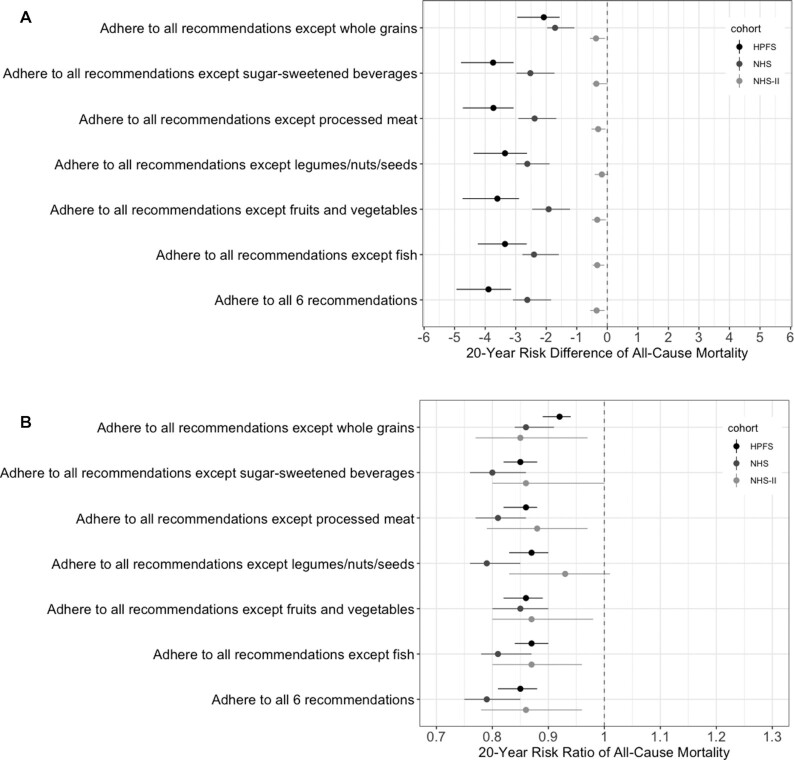
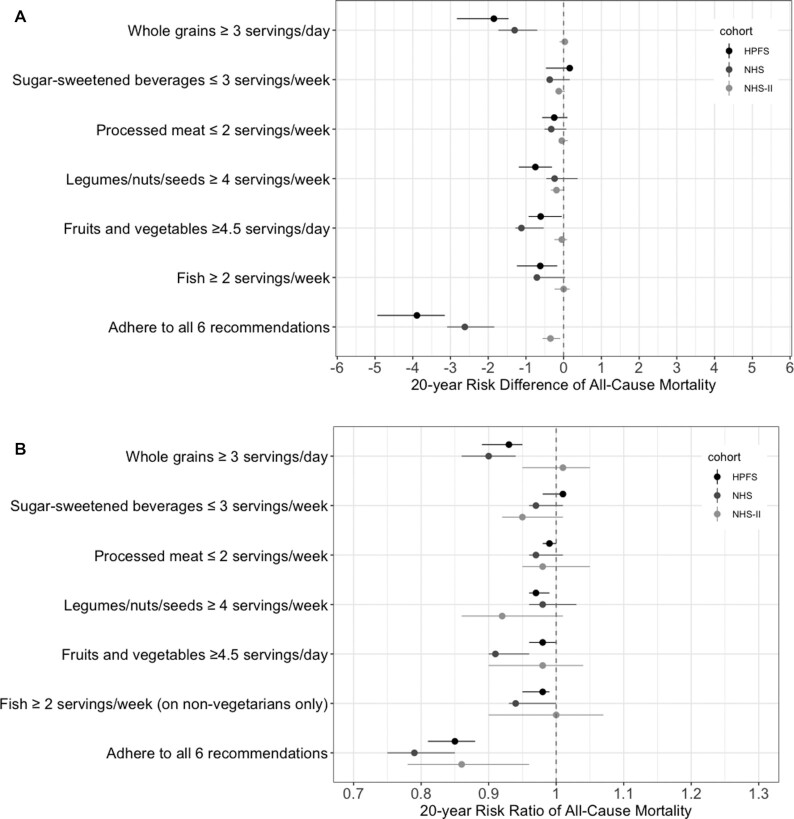
Methods: We estimated the 20-y risk of all-cause mortality under the sustained implementation of the food-based goals of the American Heart Association (AHA) 2020 using data from 3 prospective observational studies of US men [Health Professionals Follow-up Study (HPFS)] and women [Nurses' Health Study (NHS) and Nurses' Health Study II (NHS II)]. We applied the parametric g-formula to estimate the 20-y mortality risk under a dietary intervention and under no dietary intervention.
Results: There were 165,411 participants who met the eligibility criteria. The mean age at baseline was 57.4 y (range, 43-82 y) in the HPFS, 52.4 y (range, 39-66 y) in the NHS, and 40.2 y (range, 30-50 y) in the NHS II. During 20 y of follow-up, 13,241 participants died. The estimated 20-y mortality risks under a dietary intervention versus no intervention were 21.9% compared with 25.8%, respectively, in the HPFS (risk difference, -3.9%; 95% CI: -4.9% to -3.2%); 10.0% compared with 12.6%, respectively, in the NHS (risk difference, -2.6%; 95% CI: -3.1% to -1.8%); and 2.1% compared with 2.5%, respectively, in the NHS II (risk difference, -0.35%; 95% CI: -0.56% to -0.09%). The corresponding risk ratios were 0.85 (95% CI: 0.81-0.88) in the HPFS, 0.79 (95% CI: 0.75-0.85) in the NHS, and 0.86 (95% CI: 0.78-0.96) in the NHS II.
Conclusions: We estimated that adherence to the food-based AHA 2020 Dietary Goals starting in midlife may reduce the 20-y risk of mortality.
Keywords: American Heart Association 2020 Dietary Goals; g-formula; mortality; nutritional epidemiology; target trial.
© The Author(s) 2021. Published by Oxford University Press on behalf of the American Society for Nutrition.
Figures
Comment in
-
What would the trial be? Emulating randomized dietary intervention trials to estimate causal effects with observational data.Am J Clin Nutr. 2021 Aug 2;114(2):416-417. doi: 10.1093/ajcn/nqab169. Am J Clin Nutr. 2021. PMID: 34041528 No abstract available.
References
-
- Estruch R, Ros E, Salas-Salvado J, Covas MI, Corella D, Aros F, Gomez-Gracia E, Ruiz-Gutierrez V, Fiol M, Lapetra Jet al. Primary prevention of cardiovascular disease with a Mediterranean diet supplemented with extra-virgin olive oil or nuts. N Engl J Med. 2018;378(25):e34. doi:10.1056/NEJMoa1800389. - PubMed
-
- de Lorgeril M, Salen P, Martin JL, Monjaud I, Delaye J, Mamelle N. Mediterranean diet, traditional risk factors, and the rate of cardiovascular complications after myocardial infarction: final report of the Lyon Diet Heart Study. Circulation. 1999;99(6):779–85. - PubMed
-
- Esposito K, Marfella R, Ciotola M, Di Palo C, Giugliano F, Giugliano G, D'Armiento M, D'Andrea F, Giugliano D. Effect of a Mediterranean-style diet on endothelial dysfunction and markers of vascular inflammation in the metabolic syndrome: a randomized trial. JAMA. 2004;292(12):1440–6. - PubMed
-
- Shai I, Schwarzfuchs D, Henkin Y, Shahar DR, Witkow S, Greenberg I, Golan R, Fraser D, Bolotin A, Vardi Het al. Weight loss with a low-carbohydrate, Mediterranean, or low-fat diet. N Engl J Med. 2008;359(3):229–41. - PubMed
-
- Appel LJ, Moore TJ, Obarzanek E, Vollmer WM, Svetkey LP, Sacks FM, Bray GA, Vogt TM, Cutler JA, Windhauser MMet al. A clinical trial of the effects of dietary patterns on blood pressure. DASH Collaborative Research Group. N Engl J Med. 1997;336(16):1117–24. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
