

Responsiveness and minimal important change of the Pain Catastrophizing Scale in people with chronic low back pain undergoing multidisciplinary rehabilitation
- PMID: 34042409
- PMCID: PMC9980597
- DOI: 10.23736/S1973-9087.21.06729-0
Responsiveness and minimal important change of the Pain Catastrophizing Scale in people with chronic low back pain undergoing multidisciplinary rehabilitation
Abstract
Background: The Pain Catastrophizing Scale (PCS), a widely used tool to assess catastrophizing related to spinal disorders, shows valid psychometric properties in general but the minimal important change (MIC) is still not determined.
Aim: The aim of this study was to assess responsiveness and MIC of the PCS in individuals with chronic low back pain (LBP) undergoing multidisciplinary rehabilitation.
Design: Prospective observational study.
Setting: The setting was outpatient rehabilitation hospital.
Population: Two hundred and five patients with chronic LBP.
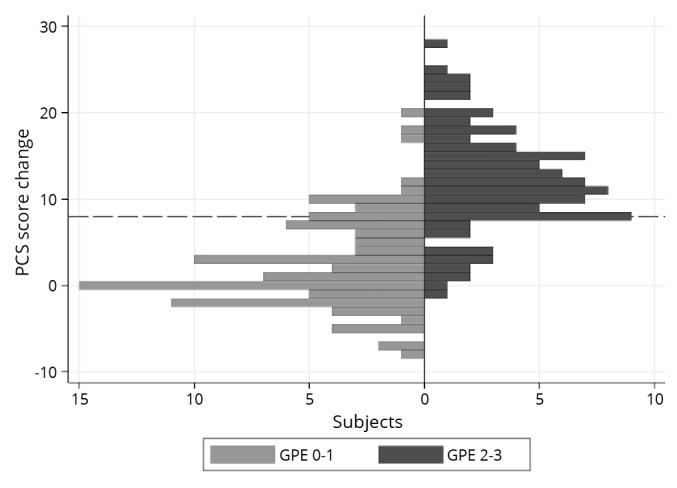
Methods: Before and after an 8-week multidisciplinary rehabilitation program, 205 patients completed the Italian version of the PCS (PCS-I). We calculated the PCS-I responsiveness by distribution-based methods (effect size [ES], standardized response mean [SRM], and minimum detectable change [MDC]) and anchor-based methods [receiver operating characteristic (ROC) curves]. After the program, participants completed a 7-point global perceived effect scale (GPE), based on which they were classified as "improved" vs. "stable." ROC curves computed the best cut-off level (taken as the MIC) between the two groups. ROC analysis was also performed on subgroups according to patients' baseline PCS scores.
Results: ES, SRM and MDC were 0.71, 0.67 and 7.73, respectively. ROC analysis yielded an MIC of 8 points (95% confidence interval [CI]: 6-10; area under the curve [AUC]: 0.88). ROC analysis of the PCS subgroups confirmed an MIC of 8 points (95%CI: 6-10) for no/low catastrophizers (score <30, N.=159; AUC: 0.90) and indicated an MIC of 11 points (95%CI: 8-14) for catastrophizers (score >30, N.=33; AUC: 0.84).
Conclusions: The PCS-I showed good ability to detect patient-perceived clinical changes in chronic LBP postrehabilitation. The MIC values we determined provide a benchmark for assessing individual improvement in this clinical context.
Clinical rehabilitation impact: The present study calculated - in a sample of people with chronic LBP - the responsiveness and MIC of the PCS. These values increase confidence in interpreting score changes, enhancing their meaningfulness for both research and clinical contexts.
Conflict of interest statement
Figures

References
-
- Sullivan MJ, Bishop SR, Pivik J. The Pain Catastrophizing Scale: development and validation. Psychol Assess 1995;7:524–32. 10.1037/1040-3590.7.4.524 - DOI
-
- Sullivan MJ. The Pain Catastrophizing Scale – User Manual. Montreal, QC: McGill University; 1995-2009.
-
- Adams VJ, Walker B, Jepson D, et al. Measurement characteristics and clinical utility of the Pain Catastrophizing Scale in individuals experiencing low back pain. Arch Phys Med Rehabil 2017;98:2350–1. 10.1016/j.apmr.2017.03.005 - DOI
-
- Terwee CB, Dekker FW, Wiersinga WM, Prummel MF, Bossuyt PM. On assessing responsiveness of health-related quality of life instruments: guidelines for instrument evaluation. Qual Life Res 2003;12:349–62. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&l... 10.1023/A:1023499322593 - DOI - PubMed
-
- Revicki D, Hays RD, Cella D, Sloan J. Recommended methods for determining responsiveness and minimally important differences for patient-reported outcomes. J Clin Epidemiol 2008;61:102–9. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&l... 10.1016/j.jclinepi.2007.03.012 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous