

Racial/Ethnic Disparities and Barriers to Diabetic Retinopathy Screening in Youths
- PMID: 34042939
- PMCID: PMC8160913
- DOI: 10.1001/jamaophthalmol.2021.1551
Racial/Ethnic Disparities and Barriers to Diabetic Retinopathy Screening in Youths
Abstract
Importance: Diabetic retinopathy is a major complication of diabetes for which regular screening improves visual health outcomes, yet adherence to screening is suboptimal.
Objective: To assess disparities in diabetic eye examination completion rates and evaluate barriers in those not previously screened.
Design, setting, and participants: In this cohort study at a single academic center (Johns Hopkins Hospital pediatric diabetes center in Baltimore, Maryland) from December 2018 to November 2019, youths with type 1 or type 2 diabetes who met criteria for diabetic retinopathy screening and were enrolled in a prospective observational trial implementing point-of-care diabetic retinopathy screening were asked about prior diabetic retinopathy screening.
Main outcomes and measures: Demographic and clinical characteristics were compared between those who did and did not have a previous diabetic eye examination and stratified according to race/ethnicity, using t tests and χ2 tests. Multivariate logistic regression was used to analyze the association between race/ethnicity, screening, and other social determinants of health. A questionnaire assessing barriers to screening adherence was administered.
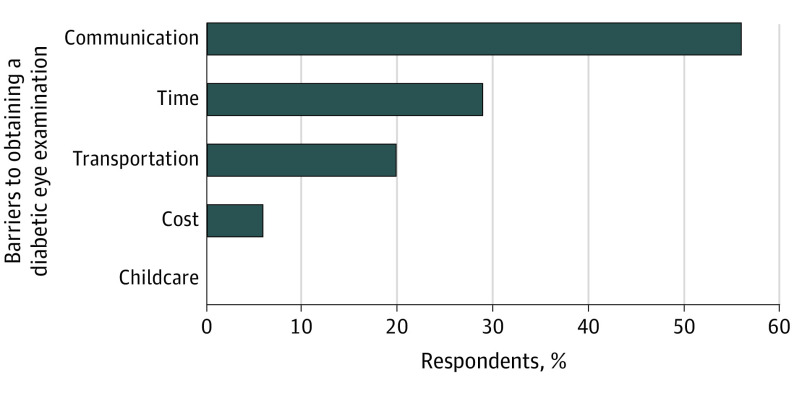
Results: Of 149 participants (76 male patients [51.0%]; mean [SD] age, 14.5 [2.3] years), 51 (34.2%) had not had a prior diabetic eye examination. These individuals were more likely than those who had prior diabetic eye examinations to be non-White youths (38 [75%] vs 31 [32%]; P < .001) and have type 2 diabetes (38 [75%] vs 10 [10%]; P < .001), Medicaid or public insurance (43 [84%] vs 31 [32%]; P < .001), lower household income (annual income ≤$25 000, 21 [41%] vs 9 [9%]; P < .001), and parents with education levels of high school or less (29 [67%] vs 22 [35%]; P < .001). The main barriers reported included not recalling being recommended to obtain a diabetic eye examination (19 [56%]), difficulty finding time for an additional appointment (10 [29%]), and transportation issues (7 [20%]). Minority youths were less likely to have a previous diabetic eye examination (non-White, 34 [46%] vs White, 64 [85%]; P < .001) and more likely to have diabetic retinopathy (11 [15%] v 2 [3%]; P = .008). Minority youths were less likely to get diabetic eye examinations even after adjusting for insurance, household income, and parental education level (odds ratio, 0.29 [95% CI, 0.10-0.79]; P = .02).
Conclusions and relevance: In this cohort study, non-White youths were less likely to undergo diabetic eye examinations yet more likely to have diabetic retinopathy compared with White youths. Addressing barriers to diabetic retinopathy screening may improve access to diabetic eye examination and facilitate early detection.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
