

Prevalence of Clinical and Subclinical Myocarditis in Competitive Athletes With Recent SARS-CoV-2 Infection: Results From the Big Ten COVID-19 Cardiac Registry
- PMID: 34042947
- PMCID: PMC8160916
- DOI: 10.1001/jamacardio.2021.2065
Prevalence of Clinical and Subclinical Myocarditis in Competitive Athletes With Recent SARS-CoV-2 Infection: Results From the Big Ten COVID-19 Cardiac Registry
Abstract
Importance: Myocarditis is a leading cause of sudden death in competitive athletes. Myocardial inflammation is known to occur with SARS-CoV-2. Different screening approaches for detection of myocarditis have been reported. The Big Ten Conference requires comprehensive cardiac testing including cardiac magnetic resonance (CMR) imaging for all athletes with COVID-19, allowing comparison of screening approaches.
Objective: To determine the prevalence of myocarditis in athletes with COVID-19 and compare screening strategies for safe return to play.
Design, setting, and participants: Big Ten COVID-19 Cardiac Registry principal investigators were surveyed for aggregate observational data from March 1, 2020, through December 15, 2020, on athletes with COVID-19. For athletes with myocarditis, presence of cardiac symptoms and details of cardiac testing were recorded. Myocarditis was categorized as clinical or subclinical based on the presence of cardiac symptoms and CMR findings. Subclinical myocarditis classified as probable or possible myocarditis based on other testing abnormalities. Myocarditis prevalence across universities was determined. The utility of different screening strategies was evaluated.
Exposures: SARS-CoV-2 by polymerase chain reaction testing.
Main outcome and measure: Myocarditis via cardiovascular diagnostic testing.
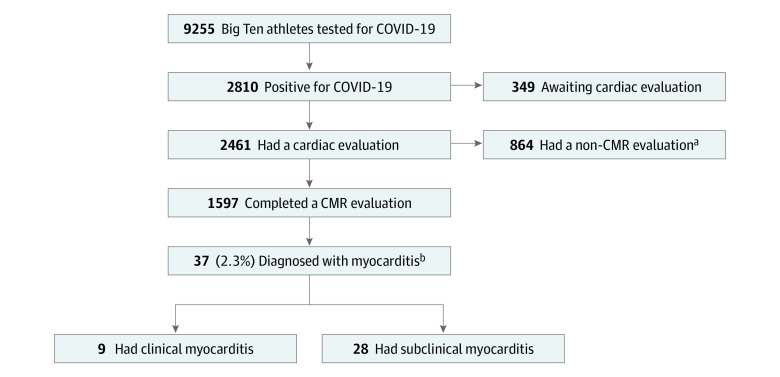
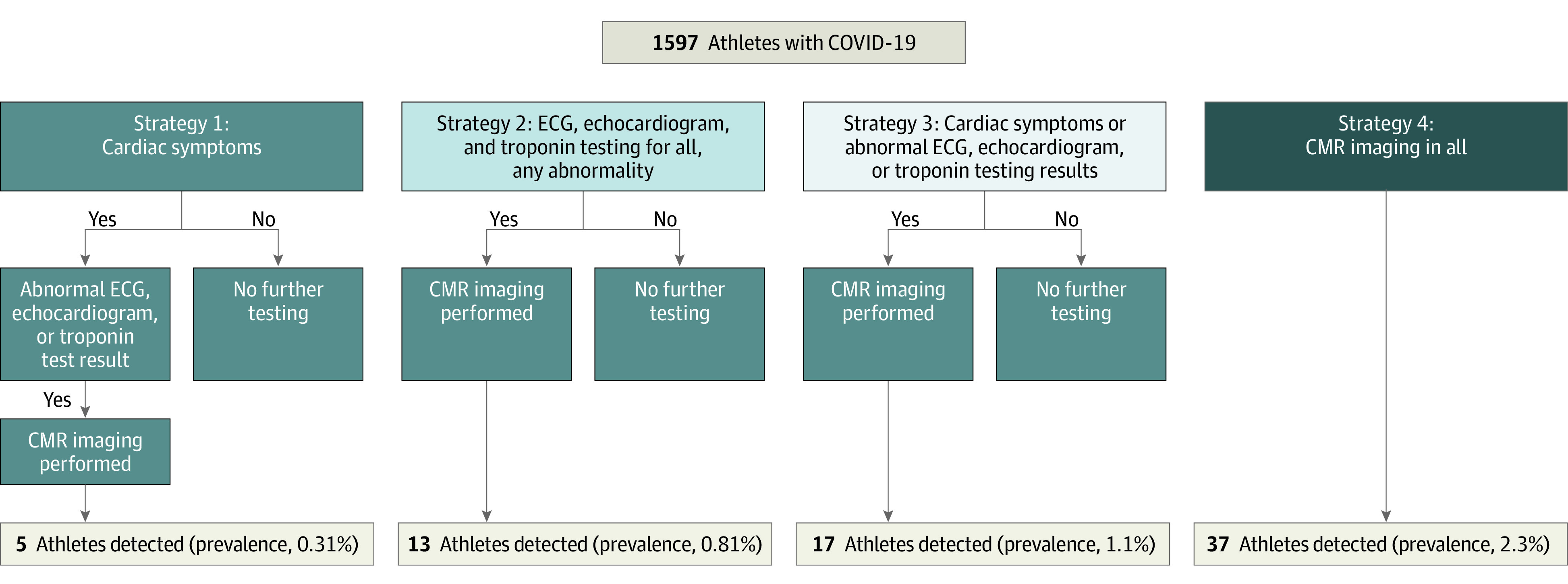
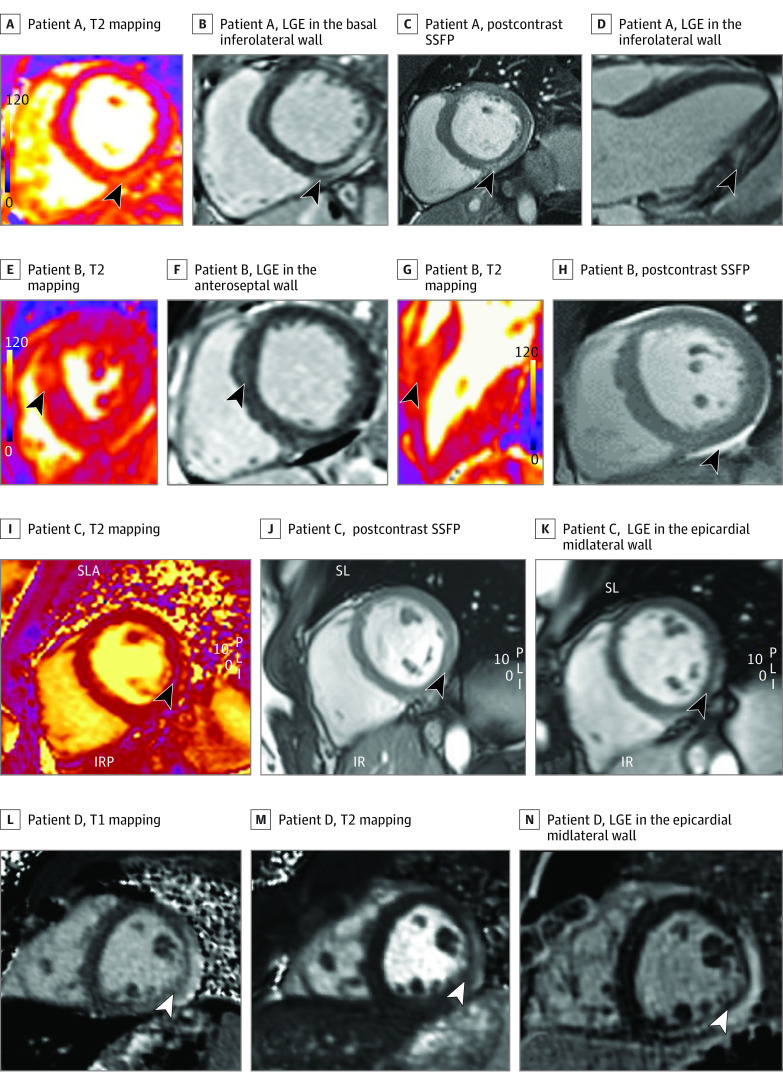
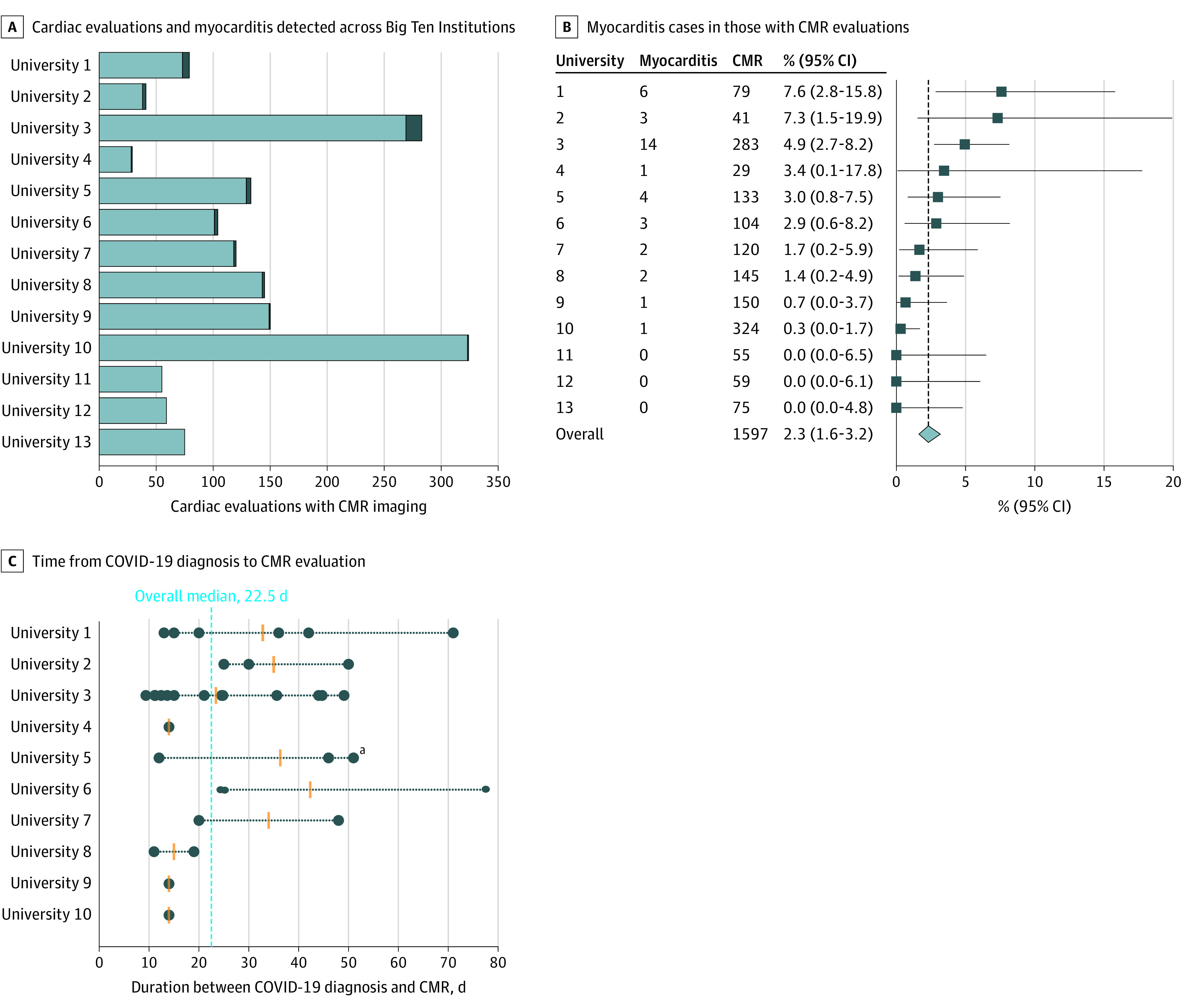
Results: Representing 13 universities, cardiovascular testing was performed in 1597 athletes (964 men [60.4%]). Thirty-seven (including 27 men) were diagnosed with COVID-19 myocarditis (overall 2.3%; range per program, 0%-7.6%); 9 had clinical myocarditis and 28 had subclinical myocarditis. If cardiac testing was based on cardiac symptoms alone, only 5 athletes would have been detected (detected prevalence, 0.31%). Cardiac magnetic resonance imaging for all athletes yielded a 7.4-fold increase in detection of myocarditis (clinical and subclinical). Follow-up CMR imaging performed in 27 (73.0%) demonstrated resolution of T2 elevation in all (100%) and late gadolinium enhancement in 11 (40.7%).
Conclusions and relevance: In this cohort study of 1597 US competitive athletes with CMR screening after COVID-19 infection, 37 athletes (2.3%) were diagnosed with clinical and subclinical myocarditis. Variability was observed in prevalence across universities, and testing protocols were closely tied to the detection of myocarditis. Variable ascertainment and unknown implications of CMR findings underscore the need for standardized timing and interpretation of cardiac testing. These unique CMR imaging data provide a more complete understanding of the prevalence of clinical and subclinical myocarditis in college athletes after COVID-19 infection. The role of CMR in routine screening for athletes safe return to play should be explored further.
Conflict of interest statement
Figures
Comment in
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
