

Cluster Analysis of Care Pathways in Adults with Major Depressive Disorder with Acute Suicidal Ideation or Behavior in the USA
- PMID: 34043148
- PMCID: PMC8166679
- DOI: 10.1007/s40273-021-01042-5
Cluster Analysis of Care Pathways in Adults with Major Depressive Disorder with Acute Suicidal Ideation or Behavior in the USA
Abstract
Background and objective: Suicidal ideation or behavior are core symptoms of major depressive disorder (MDD). This study aimed to understand heterogeneity among patients with MDD and acute suicidal ideation or behavior.
Methods: Adults with a diagnosis of MDD on the same day or 6 months before a claim for suicidal ideation or behavior (index date) were identified in the MarketScan® Databases (10/01/2014-04/30/2019). A mathematical algorithm was used to cluster patients on characteristics of care measured pre-index. Patient care pathways were described by cluster during the 12-month pre-index period and up to 12 months post-index.
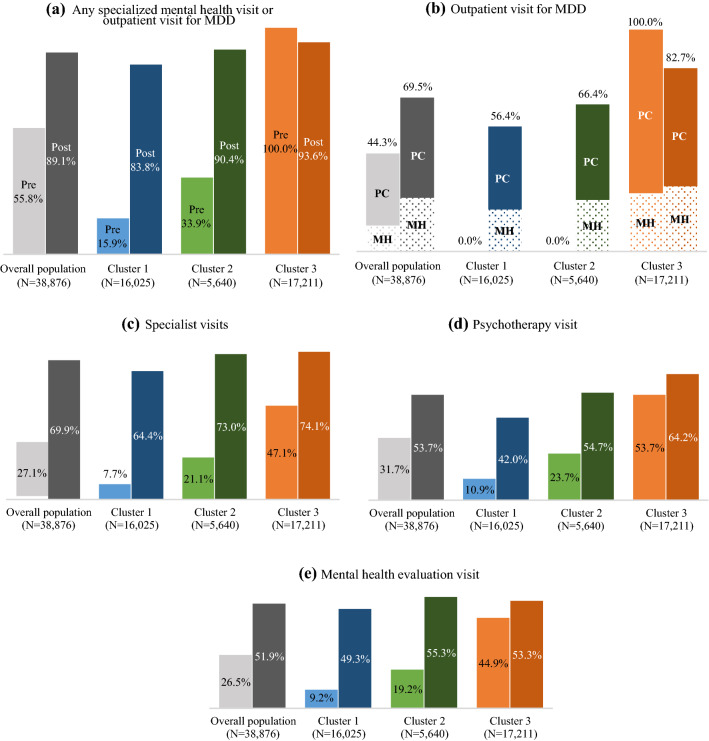
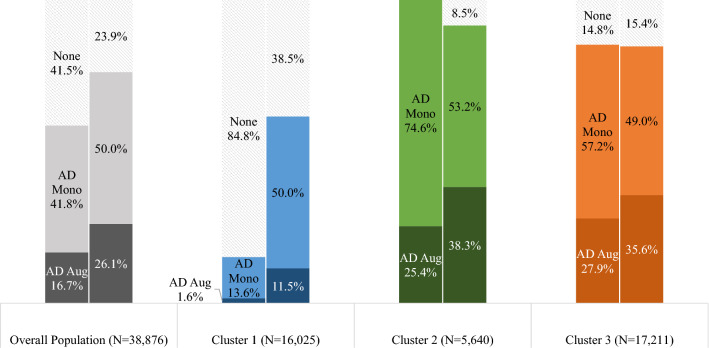
Results: Among 38,876 patients with MDD and acute suicidal ideation or behavior, three clusters were identified. Across clusters, pre-index exposure to mental healthcare was revealed as a key differentiator: Cluster 1 (N = 16,025) was least exposed, Cluster 2 (N = 5640) moderately exposed, and Cluster 3 (N = 17,211) most exposed. Patients whose MDD diagnosis was first observed during their index event comprised 86.0% and 72.8% of Clusters 1 and 2, respectively; in Cluster 3, all patients had an MDD diagnosis pre-index. Within 30 days post-index, in Clusters 1, 2, and 3, respectively, 79.3%, 85.2%, and 88.2% used mental health services, including outpatient visits for MDD. Within 12 months post-index, 61.5%, 91.5%, and 84.6% had one or more antidepressant claim, respectively. Per-patient index event costs averaged $5614, $6645, and $5853, respectively.
Conclusions: Patients with MDD and acute suicidal ideation or behavior least exposed to the healthcare system pre-index similarly received the least care post-index. An opportunity exists to optimize treatment and follow-up with mental health services.
Conflict of interest statement
Jennifer Voelker, Abigail I. Nash, Kruti Joshi, and Cheryl Neslusan are employees of Janssen Scientific Affairs, LLC, and are stockholders of Johnson & Johnson. Maryia Zhdanava, Dominic Pilon, Tom Cornwall, Laura Morrison, Maude Vermette-Laforme, and Patrick Lefebvre are employees of Analysis Group, Inc., a consulting company that has provided paid consulting services to Janssen Scientific Affairs, LLC, which funded the development and conduct of this study and article.
Figures




Similar articles
-
Esketamine nasal spray for major depressive disorder with acute suicidal ideation or behavior: description of treatment access, utilization, and claims-based outcomes in the United States.J Med Econ. 2023 Jan-Dec;26(1):691-700. doi: 10.1080/13696998.2023.2208993. J Med Econ. 2023. PMID: 37130075
-
Excess healthcare resource utilization and healthcare costs among privately and publicly insured patients with major depressive disorder and acute suicidal ideation or behavior in the United States.J Affect Disord. 2022 Aug 15;311:303-310. doi: 10.1016/j.jad.2022.05.086. Epub 2022 May 18. J Affect Disord. 2022. PMID: 35597466
-
Clinical and economic burden of major depressive disorder with acute suicidal ideation or behavior in a US Veterans Health Affairs database.Curr Med Res Opin. 2022 Sep;38(9):1603-1611. doi: 10.1080/03007995.2022.2081452. Epub 2022 Jun 30. Curr Med Res Opin. 2022. PMID: 35670276
-
A Southeast Asian expert consensus on the management of major depressive disorder with suicidal behavior in adults under 65 years of age.BMC Psychiatry. 2022 Jul 21;22(1):489. doi: 10.1186/s12888-022-04140-6. BMC Psychiatry. 2022. PMID: 35864465 Free PMC article. Review.
-
Major depressive disorder with suicidal ideation or behavior in Chinese population: A scoping review of current evidence on disease assessment, burden, treatment and risk factors.J Affect Disord. 2023 Nov 1;340:732-742. doi: 10.1016/j.jad.2023.08.106. Epub 2023 Aug 22. J Affect Disord. 2023. PMID: 37619652
Cited by
-
The Growing Burden of Major Depressive Disorders (MDD): Implications for Researchers and Policy Makers.Pharmacoeconomics. 2021 Jun;39(6):619-625. doi: 10.1007/s40273-021-01040-7. Epub 2021 May 20. Pharmacoeconomics. 2021. PMID: 34013439 Free PMC article. No abstract available.
-
Exploring risk factors for re-hospitalization in a psychiatric inpatient setting: a retrospective naturalistic study.BMC Psychiatry. 2022 Dec 22;22(1):821. doi: 10.1186/s12888-022-04472-3. BMC Psychiatry. 2022. PMID: 36550540 Free PMC article.
-
A framework for inferring and analyzing pharmacotherapy treatment patterns.BMC Med Inform Decis Mak. 2024 Mar 8;24(1):68. doi: 10.1186/s12911-024-02469-4. BMC Med Inform Decis Mak. 2024. PMID: 38459459 Free PMC article.
-
Profiles, Correlates and Outcomes Among Patients Experiencing an Onset of Mental Disorder Based on Outpatient Care Received Following Index Emergency Department Visits.Can J Psychiatry. 2022 Oct;67(10):787-801. doi: 10.1177/07067437221087004. Epub 2022 Mar 15. Can J Psychiatry. 2022. PMID: 35289196 Free PMC article.
References
-
- Substance Abuse and Mental Health Services Administration (SAMHSA). National survey on drug use and health: key substance use and mental health indicators in the United States. 2019. https://www.samhsa.gov/data/sites/default/files/reports/rpt29393/2019NSD.... Accessed 3 Mar 2021.
-
- GBD 2017 Disease Injury Incidence Prevalence Collaborators Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1789–1858. doi: 10.1016/S0140-6736(18)32279-7. - DOI - PMC - PubMed
-
- World Health Organization. Depression: key facts. 2020. http://www.who.int/mediacentre/factsheets/fs369/en/. Accessed 7 Oct 2020.
-
- American Psychiatric Association. Practice guideline for the treatment of patients with major depressive disorder. Third Edition. 2010. https://psychiatryonline.org/pb/assets/raw/sitewide/practice_guidelines/.... Accessed 27 Jun 2018.
-
- Kuvadia H, Wang K, Daly E, Voelker J, Pesa J, Connolly N, et al. National trends in the prevalence of major depressive disorder with suicidal ideation among adults using the National Survey on Drug Use and Health. Annual Psych Congress; 30-6 Oct 2019; San Diego (CA).
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
