

Laparotomic versus robotic surgery in elderly patients with endometrial cancer: A systematic review and meta-analysis
- PMID: 34043235
- PMCID: PMC9292514
- DOI: 10.1002/ijgo.13766
Laparotomic versus robotic surgery in elderly patients with endometrial cancer: A systematic review and meta-analysis
Abstract
Background: Although robotics has been shown to improve outcomes in some high-difficulty surgical category patients, it is unclear if such an approach may improve outcomes in elderly patients with endometrial carcinoma (EC).
Objective: To compare robotic and laparotomic surgery in the treatment and staging of elderly EC patients.
Materials and methods: A systematic review and meta-analysis was performed assessing the risk of overall, intra-operative, and peri-operative complications associated with the surgical approach (laparotomic vs robotic) for elderly patients with EC by relative risk (RR). Pooled means ± standard deviation of length of stay were compared with the unpaired t test. Subgroup analyses for overall complications were performed based on different age cut-offs (>70, >65, and >75 years) and severity of complications (minor and major). A value of P less than 0.05 was considered significant.
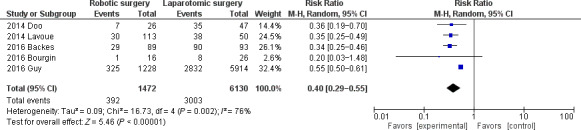
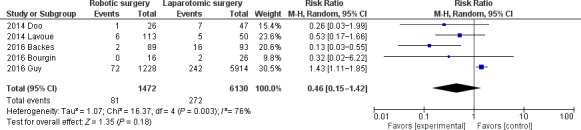
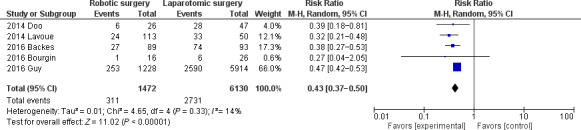
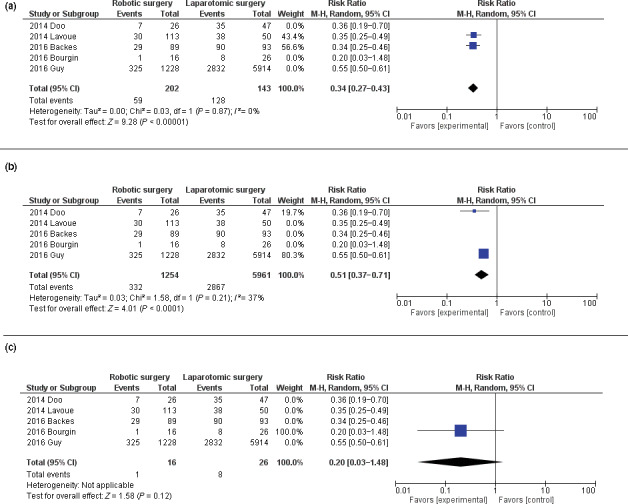
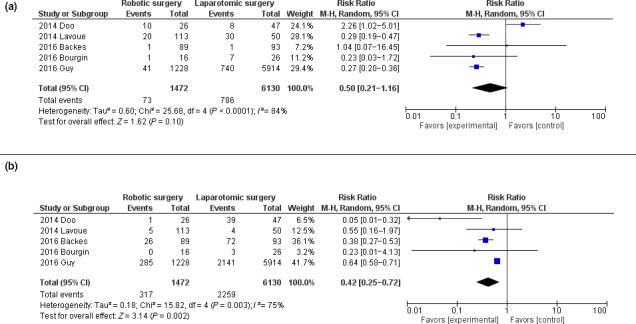
Results: Five studies with 7629 EC patients were included. Pooled RR for robotic compared with laparotomic surgery was 0.40 (P < 0.001) for overall, 0.46 (P = 0.18) for intra-operative, and 0.43 (P < 0.001) for peri-operative complications. Pooled difference between means ± standard deviation of length of stay for robotic versus laparotomic surgery was -3.34 (P < 0.001). At subgroup analyses, pooled RR of overall complications for robotic surgery versus laparotomic surgery was 0.34 (P < 0.001) in the >70 years, 0.51 (P < 0.01) in the >65 years, 0.20 (P = 0.12) in the >75 years groups. Pooled RR was 0.50 (P = 0.1) in the minor complications subgroup, and 0.42 (P = 0.002) in the major complications subgroup.
Conclusion: Robotics might be a viable alternative to the laparotomic approach for EC in elderly patients because it significantly decreases the risk of overall and peri-operative complications (mainly major complications), and the length of stay when compared with laparotomy. The decrease in risk of overall complications is greater with increasing patient age.
Keywords: cancer; endometrium; laparotomy; robotics; surgery; tumor.
© 2021 The Authors. International Journal of Gynecology & Obstetrics published by John Wiley & Sons Ltd on behalf of International Federation of Gynecology and Obstetrics.
Conflict of interest statement
The authors have no conflicts of interest.
Figures

Similar articles
-
Intravenous versus inhalational maintenance of anaesthesia for postoperative cognitive outcomes in elderly people undergoing non-cardiac surgery.Cochrane Database Syst Rev. 2018 Aug 21;8(8):CD012317. doi: 10.1002/14651858.CD012317.pub2. Cochrane Database Syst Rev. 2018. PMID: 30129968 Free PMC article.
-
Pre-operative endometrial thinning agents before endometrial destruction for heavy menstrual bleeding.Cochrane Database Syst Rev. 2002;(3):CD001124. doi: 10.1002/14651858.CD001124. Cochrane Database Syst Rev. 2002. Update in: Cochrane Database Syst Rev. 2014 Jul 29;(7):CD001124. doi: 10.1002/14651858.CD001124.pub2. PMID: 12137619 Updated.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of topotecan for ovarian cancer.Health Technol Assess. 2001;5(28):1-110. doi: 10.3310/hta5280. Health Technol Assess. 2001. PMID: 11701100
-
Robotic-assisted hysterectomy for endometrial cancer compared with traditional laparoscopic and laparotomy approaches: a systematic review.Obstet Gynecol. 2010 Dec;116(6):1422-1431. doi: 10.1097/AOG.0b013e3181f74153. Obstet Gynecol. 2010. PMID: 21099613
-
Electronic cigarettes for smoking cessation.Cochrane Database Syst Rev. 2022 Nov 17;11(11):CD010216. doi: 10.1002/14651858.CD010216.pub7. Cochrane Database Syst Rev. 2022. Update in: Cochrane Database Syst Rev. 2024 Jan 8;1:CD010216. doi: 10.1002/14651858.CD010216.pub8. PMID: 36384212 Free PMC article. Updated.
Cited by
-
Outcome of robot-assisted surgery for stage IA endometrial cancer compared to open and laparoscopic surgeries: a retrospective study at a single institution.J Robot Surg. 2024 Mar 23;18(1):133. doi: 10.1007/s11701-024-01897-8. J Robot Surg. 2024. PMID: 38520654
-
Robotic Surgery in Severely Obese Frail Patients for the Treatment of Atypical Endometrial Hyperplasia and Endometrial Cancer: A Propensity-Match Analysis at an ESGO-Accredited Center.Cancers (Basel). 2025 Feb 1;17(3):482. doi: 10.3390/cancers17030482. Cancers (Basel). 2025. PMID: 39941849 Free PMC article.
-
Different surgical methods of hysterectomy for the management of endometrial cancer: a systematic review and network meta-analysis.Front Oncol. 2025 Jan 15;14:1524991. doi: 10.3389/fonc.2024.1524991. eCollection 2024. Front Oncol. 2025. PMID: 39882446 Free PMC article.
-
Surgery Advances in Gynecologic Tumors: The Evolution and Outcomes of Robotic Surgery for Gynecologic Cancers in a Tertiary Center.Curr Oncol. 2024 Apr 24;31(5):2400-2409. doi: 10.3390/curroncol31050179. Curr Oncol. 2024. PMID: 38785460 Free PMC article. Review.
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015. CA Cancer J Clin. 2015;65(1):5‐29. - PubMed
-
- Raffone A, Travaglino A, Mascolo M, et al. TCGA molecular groups of endometrial cancer: pooled data about prognosis. Gynecol Oncol. 2019;155(2):374‐383. - PubMed
-
- Travaglino A, Raffone A, Mascolo M, et al. TCGA molecular subgroups in endometrial undifferentiated/dedifferentiated carcinoma. PatholOncol Res. 2020;26(3):1411‐1416. - PubMed
-
- Raffone A, Travaglino A, Mascolo M, et al. Histopathological characterization of ProMisE molecular groups of endometrial cancer. Gynecol Oncol. 2020;157(1):252‐259. - PubMed
-
- Raffone A, Troisi J, Boccia D, et al. Metabolomics in endometrial cancer diagnosis: a systematic review. Acta Obstet Gynecol Scand. 2020;99(9):1135‐1146. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
