

NanoString technology distinguishes anti-TIF-1γ+ from anti-Mi-2+ dermatomyositis patients
- PMID: 34043263
- PMCID: PMC8412076
- DOI: 10.1111/bpa.12957
NanoString technology distinguishes anti-TIF-1γ+ from anti-Mi-2+ dermatomyositis patients
Erratum in
-
Corrigendum.Brain Pathol. 2022 Mar;32(2):e13053. doi: 10.1111/bpa.13053. Brain Pathol. 2022. PMID: 35213085 Free PMC article. No abstract available.
Abstract
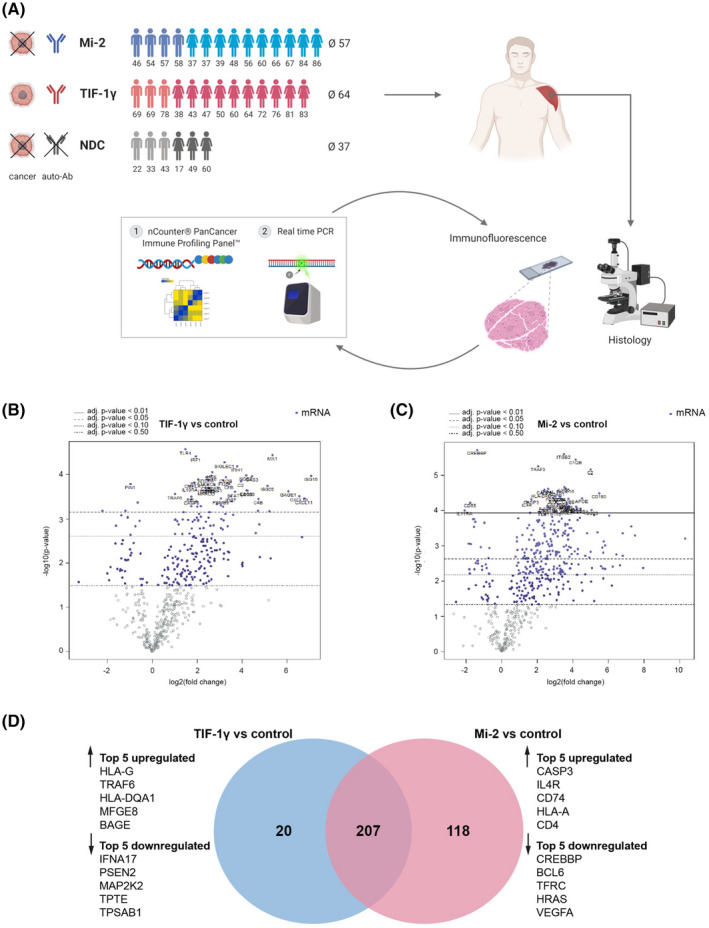
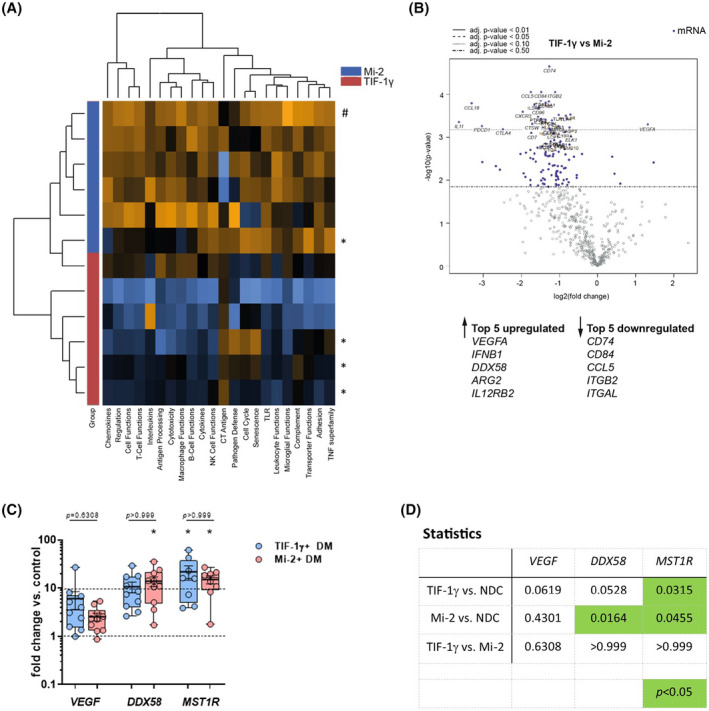
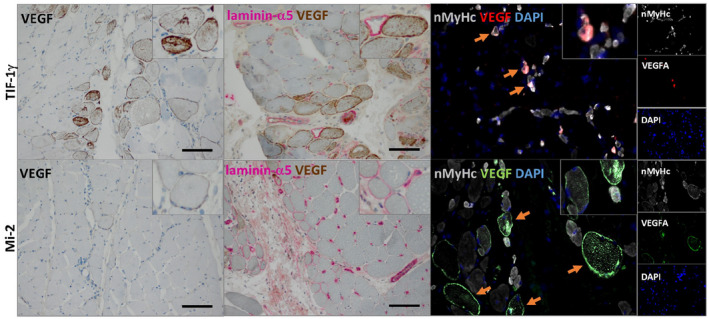
Dermatomyositis (DM) is a systemic idiopathic inflammatory disease affecting skeletal muscle and skin, clinically characterized by symmetrical proximal muscle weakness and typical skin lesions. Recently, myositis-specific autoantibodies (MSA) became of utmost importance because they strongly correlate with distinct clinical manifestations and prognosis. Antibodies against transcription intermediary factor 1γ (TIF-1γ) are frequently associated with increased risk of malignancy, a specific cutaneous phenotype and limited response to therapy in adult DM patients. Anti-Mi-2 autoantibodies, in contrast, are typically associated with classic DM rashes, prominent skeletal muscle weakness, better therapeutic response and prognosis, and less frequently with cancer. Nevertheless, the sensitivity of autoantibody testing is only moderate, and alternative reliable methods for DM patient stratification and prediction of cancer risk are needed. To further investigate these clinically distinct DM subgroups, we herein analyzed 30 DM patients (n = 15 Mi-2+ and n = 15 TIF-1 γ+ ) and n = 8 non-disease controls (NDC). We demonstrate that the NanoString technology can be used as a very sensitive method to clearly differentiate these two clinically distinct DM subgroups. Using the nCounter PanCancer Immune Profiling Panel™, we identified a set of significantly dysregulated genes in anti-TIF-1γ+ patient muscle biopsies including VEGFA, DDX58, IFNB1, CCL5, IL12RB2, and CD84. Investigation of type I IFN-regulated transcripts revealed a striking type I interferon signature in anti-Mi-2+ patient biopsies. Our results help to stratify both subgroups and predict, which DM patients require an intensified diagnostic procedure and might have a poorer outcome. Potentially, this could also have implications for the therapeutic approach.
Keywords: Mi-2; NanoString; TIF-1γ; dermatomyositis; myositis-specific antibody; skeletal muscle.
© 2021 The Authors. Brain Pathology published by John Wiley & Sons Ltd on behalf of International Society of Neuropathology.
Conflict of interest statement
The authors report no disclosures relevant to the manuscript.
Figures
References
-
- Mammen AL, Allenbach Y, Stenzel W, Benveniste O, ENMC 239th Workshop Study Group . 239th ENMC International Workshop: Classification of dermatomyositis, Amsterdam, the Netherlands, 14–16 December 2018. Neuromuscul Disord. 2020;30:70–92. - PubMed
-
- Sasaki H, Kohsaka H. Current diagnosis and treatment of polymyositis and dermatomyositis. Mod Rheumatol. 2018;28:913–21. - PubMed
-
- Hida A, Yamashita T, Hosono Y, Inoue M, Kaida K, Kadoya M, et al. Anti‐TIF1‐gamma antibody and cancer‐associated myositis: A clinicohistopathologic study. Neurology. 2016;87:299–308. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
