

Association between longitudinal blood pressure and prognosis after treatment of cerebral aneurysm: A nationwide population-based cohort study
- PMID: 34043701
- PMCID: PMC8158927
- DOI: 10.1371/journal.pone.0252042
Association between longitudinal blood pressure and prognosis after treatment of cerebral aneurysm: A nationwide population-based cohort study
Abstract
Background: High blood pressure is a major risk factor for the development and rupture of cerebral aneurysm. Endovascular coil embolization and surgical clipping are established procedures to treat cerebral aneurysm. However, longitudinal data of blood pressure after the treatment of cerebral aneurysm and its impact on long-term prognosis are not well known.
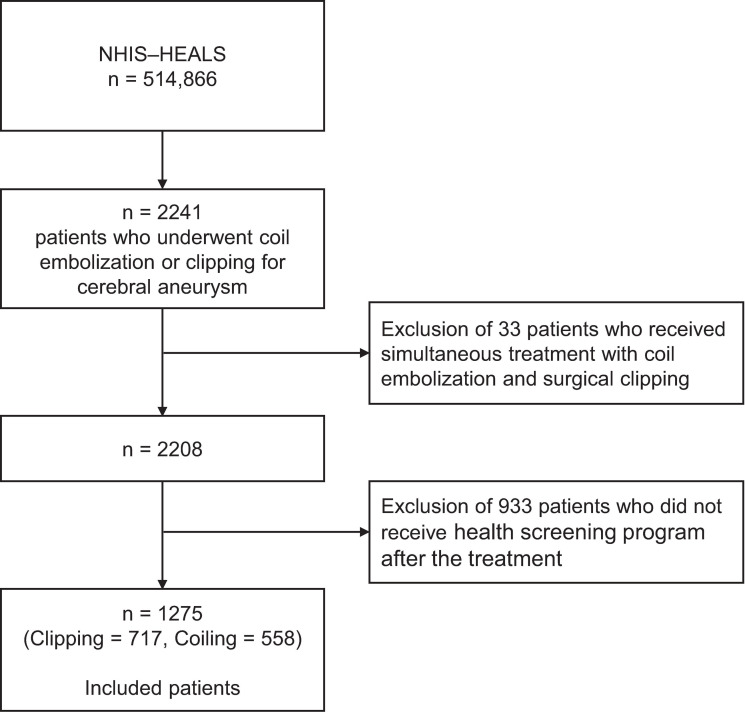
Methods: This retrospective cohort study included 1275 patients who underwent endovascular coil embolization (n = 558) or surgical clipping (n = 717) of cerebral aneurysm in 2002-2015 using the nationwide health screening database of Korea. Systolic and diastolic blood pressure of patients were repeatedly obtained from the nationwide health screening program. We performed a multivariate time-dependent Cox regression analysis of the primary composite outcome of stroke, myocardial infarction, and all-cause death.
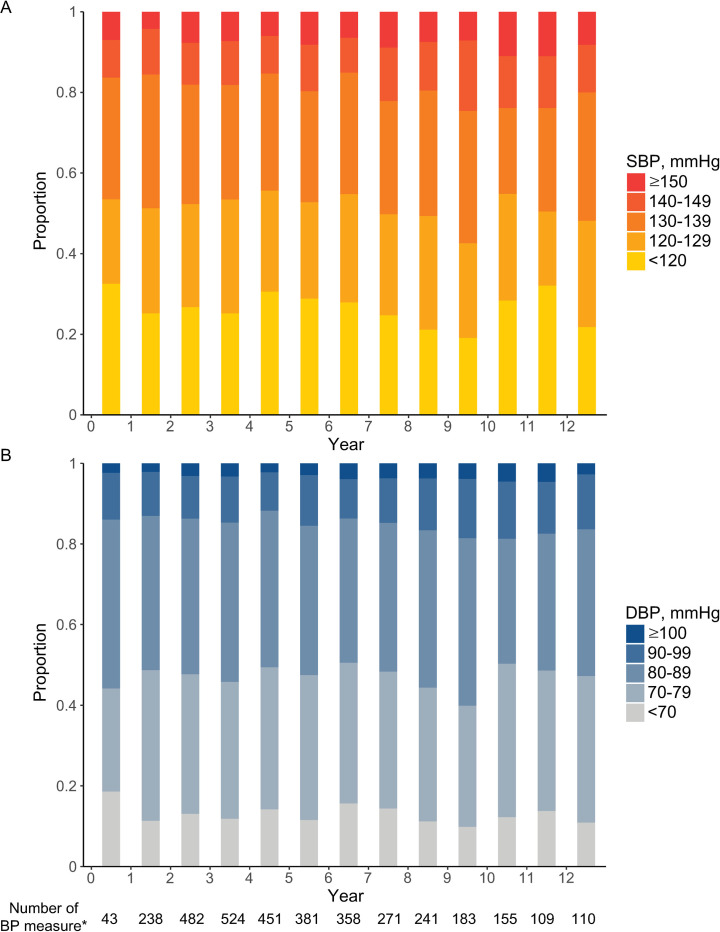
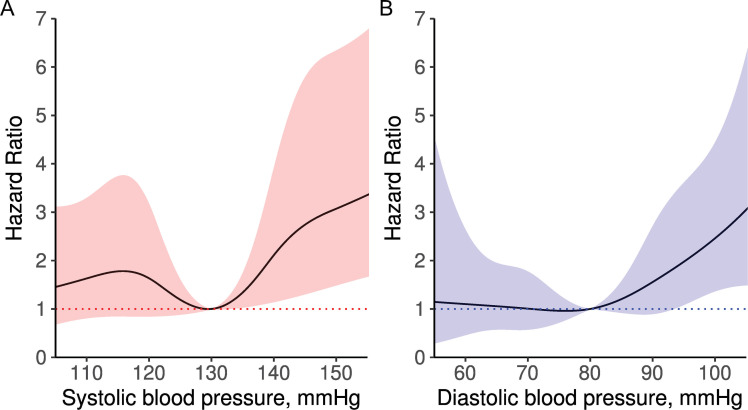
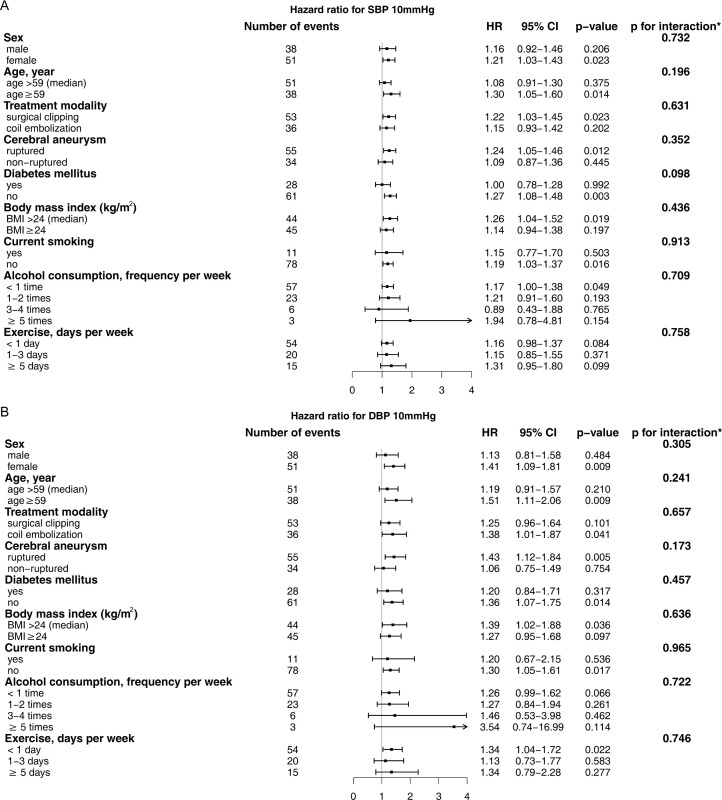
Results: During the mean follow-up period of 6.13 ± 3.41 years, 89 patients suffered the primary outcome. Among the total 3546 times of blood pressure measurement, uncontrolled high blood pressure (systolic ≥140 mmHg or diastolic ≥90 mmHg) was 22.9%. There was a significantly increased risk of primary outcome with high systolic (adjusted HR [95% CI] per 10 mmHg, 1.16 [1.01-1.35]) and diastolic (adjusted HR [95% CI] per 10 mmHg, 1.32 [1.06-1.64]) blood pressure.
Conclusions: High blood pressure is prevalent even in patients who received treatment for cerebral aneurysm, which is significantly associated with poor outcome. Strict control of high blood pressure may further improve the prognosis of patients with cerebral aneurysm.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Long-term outcomes of treatment for unruptured intracranial aneurysms in South Korea: clipping versus coiling.J Neurointerv Surg. 2018 Dec;10(12):1218-1222. doi: 10.1136/neurintsurg-2018-013757. Epub 2018 Jun 6. J Neurointerv Surg. 2018. PMID: 29875276
-
Long-term survival outcomes and prognostic factors related to ruptured intracranial aneurysms: A comparison of surgical and endovascular options in a propensity score-matched, nationwide population-based cohort study.Eur J Neurol. 2021 Sep;28(9):3012-3021. doi: 10.1111/ene.15002. Epub 2021 Jul 14. Eur J Neurol. 2021. PMID: 34192398
-
Coil embolization for intracranial aneurysms: an evidence-based analysis.Ont Health Technol Assess Ser. 2006;6(1):1-114. Epub 2006 Jan 1. Ont Health Technol Assess Ser. 2006. PMID: 23074479 Free PMC article.
-
Endovascular coiling versus neurosurgical clipping for people with aneurysmal subarachnoid haemorrhage.Cochrane Database Syst Rev. 2018 Aug 15;8(8):CD003085. doi: 10.1002/14651858.CD003085.pub3. Cochrane Database Syst Rev. 2018. PMID: 30110521 Free PMC article.
-
Endovascular coiling vs. surgical clipping for unruptured intracranial aneurysm: A meta-analysis.Br J Neurosurg. 2015;29(4):485-92. doi: 10.3109/02688697.2015.1023771. Epub 2015 Jun 3. Br J Neurosurg. 2015. PMID: 26037936
Cited by
-
Machine Learning for Predicting Thromboembolic Events Following Flow Diverter Treatment of Intracranial Aneurysms: A Multicenter Retrospective Study.Neurol Ther. 2025 Aug 27. doi: 10.1007/s40120-025-00808-9. Online ahead of print. Neurol Ther. 2025. PMID: 40866785
-
Anodal Electrical Taste Stimulation to the Chin Enhances the Salt Taste Perception in Subarachnoid Hemorrhage Patients.Cureus. 2024 Mar 21;16(3):e56630. doi: 10.7759/cureus.56630. eCollection 2024 Mar. Cureus. 2024. PMID: 38650787 Free PMC article.
-
Association of eNOS T786C genetic polymorphism with the risk of aneurysmal subarachnoid haemorrhage.Transl Neurosci. 2025 Apr 16;16(1):20250368. doi: 10.1515/tnsci-2025-0368. eCollection 2025 Jan 1. Transl Neurosci. 2025. PMID: 40292421 Free PMC article.
-
Dimethyl Fumarate Mediates Sustained Vascular Smooth Muscle Cell Remodeling in a Mouse Model of Cerebral Aneurysm.Antioxidants (Basel). 2024 Jun 27;13(7):773. doi: 10.3390/antiox13070773. Antioxidants (Basel). 2024. PMID: 39061841 Free PMC article.
-
Development of an indicator framework for assessing nursing quality in interventional therapy for intracranial aneurysms in China.Front Neurol. 2024 Dec 5;15:1403637. doi: 10.3389/fneur.2024.1403637. eCollection 2024. Front Neurol. 2024. PMID: 39703355 Free PMC article.
References
-
- Thompson BG, Brown RD, Amin-Hanjani S, et al.. Guidelines for the Management of Patients With Unruptured Intracranial Aneurysms: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke. 2015;46: 2368–2400. 10.1161/STR.0000000000000070 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
