

Pneumothorax in critically ill patients with COVID-19 infection: Incidence, clinical characteristics and outcomes in a case control multicenter study
- PMID: 34044224
- PMCID: PMC8116127
- DOI: 10.1016/j.rmed.2021.106464
Pneumothorax in critically ill patients with COVID-19 infection: Incidence, clinical characteristics and outcomes in a case control multicenter study
Abstract
Background: The clinical features and outcomes of mechanically ventilated patients with COVID-19 infection who develop a pneumothorax has not been rigorously described or compared to those who do not develop a pneumothorax.
Purpose: To determine the incidence, clinical characteristics, and outcomes of critically ill patients with COVID-19 infection who developed pneumothorax. In addition, we compared the clinical characteristics and outcomes of mechanically ventilated patients who developed a pneumothorax with those who did not develop a pneumothorax.
Methods: This study was a multicenter retrospective analysis of all adult critically ill patients with COVID-19 infection who were admitted to intensive care units in 4 tertiary care centers in the United States.
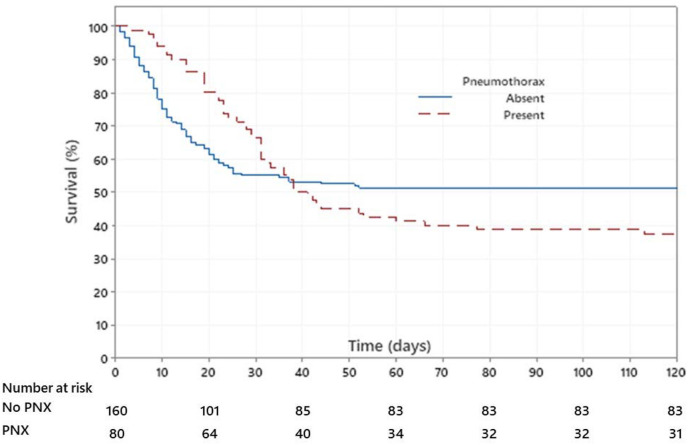
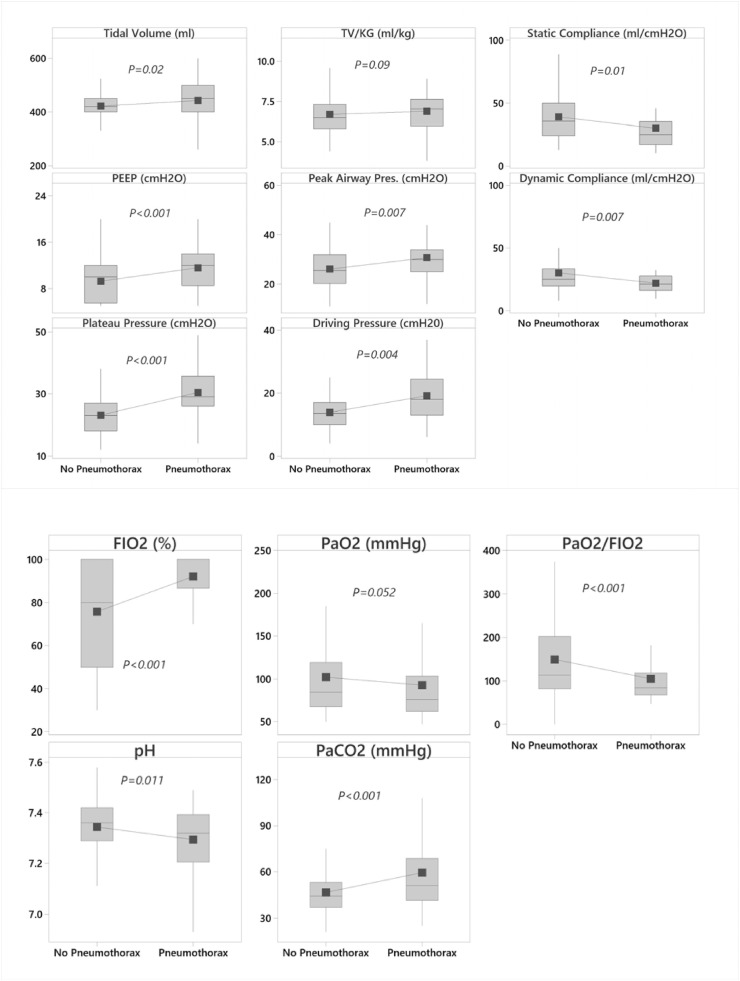
Results: A total of 842 critically ill patients with COVID-19 infection were analyzed, out of which 594 (71%) were mechanically ventilated. The overall incidence of pneumothorax was 85/842 (10%), and 80/594 (13%) in those who were mechanically ventilated. As compared to mechanically ventilated patients in the non-pneumothorax group, mechanically ventilated patients in the pneumothorax group had worse respiratory parameters at the time of intubation (mean PaO2:FiO2 ratio 105 vs 150, P<0.001 and static respiratory system compliance: 30ml/cmH2O vs 39ml/cmH2O, P = 0.01) and significantly higher in-hospital mortality (63% vs 49%, P = 0.04).
Conclusion: The overall incidence of pneumothorax in mechanically ventilated patients with COVID-19 infection was 13%. Mechanically ventilated patients with COVID-19 infection who developed pneumothorax had worse gas exchange and respiratory mechanics at the time of intubation and had a higher mortality compared to those who did not develop pneumothorax.
Keywords: 2; Barotrauma; COVID-19; Coronavirus disease 2019; Incidence; Mortality; Pneumomediastinum; Pneumothorax; SARS-CoV-2.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Conflict of interest statement
MAJ: received institution grant support from Mallinckrodt pharmaceuticals. JH: Consultant/Advisory Boards: IBIOS [IPF]; Roche/Genentech [IPF (Nintedanib)]; Boehringer Ingelheim [IPF (Pirfenidone)]. PJF: Scientific advisor with shares in Penrose TherapeuTx, LLC. The remaining authors have no disclosures or any potential conflicts of interest.
Figures
Comment in
-
Pneumothorax and barotrauma in invasively ventilated patients with COVID-19.Respir Med. 2021 Oct;187:106552. doi: 10.1016/j.rmed.2021.106552. Epub 2021 Jul 30. Respir Med. 2021. PMID: 34364198 Free PMC article. No abstract available.
References
-
- Yarmus L., Feller-Kopman D. Pneumothorax in the critically ill patient. Chest. 2012;141(4):1098–1105. - PubMed
-
- Esteban A., Anzueto A., Frutos F., et al. Characteristics and outcomes in adult patients receiving mechanical ventilation: a 28-day international study. J. Am. Med. Assoc. 2002;287(3):345–355. - PubMed
-
- Bedos J.P., Dumoulin J.L., Gachot B., et al. Pneumocystis carinii pneumonia requiring intensive care management: survival and prognostic study in 110 patients with human immunodeficiency virus. Crit. Care Med. 1999;27(6):1109–1115. - PubMed
-
- Gattinoni L., Bombino M., Pelosi P., et al. Lung structure and function in different stages of severe adult respiratory distress syndrome. J. Am. Med. Assoc. 1994;271(22):1772–1779. - PubMed
-
- Rivero A., Perez-Camacho I., Lozano F., et al. Etiology of spontaneous pneumothorax in 105 HIV-infected patients without highly active antiretroviral therapy. Eur. J. Radiol. 2009;71(2):264–268. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
