

Community-based molecular and serological surveillance of subclinical malaria in Myanmar
- PMID: 34044836
- PMCID: PMC8161608
- DOI: 10.1186/s12916-021-01993-8
Community-based molecular and serological surveillance of subclinical malaria in Myanmar
Abstract
Background: In the Greater Mekong Subregion (GMS), current malaria surveillance strategies rely on a network of village health volunteers (VHVs) reporting the results of rapid diagnostic tests (RDTs), known to miss many asymptomatic infections. Integration of more sensitive diagnostic molecular and serological measures into the VHV network may improve surveillance of residual malaria transmission in hard-to-reach areas in the region and inform targeted interventions and elimination responses. However, data on residual malaria transmission that would be captured by these measures in the VHV-led testing and treatment surveillance network in the GMS is unknown.
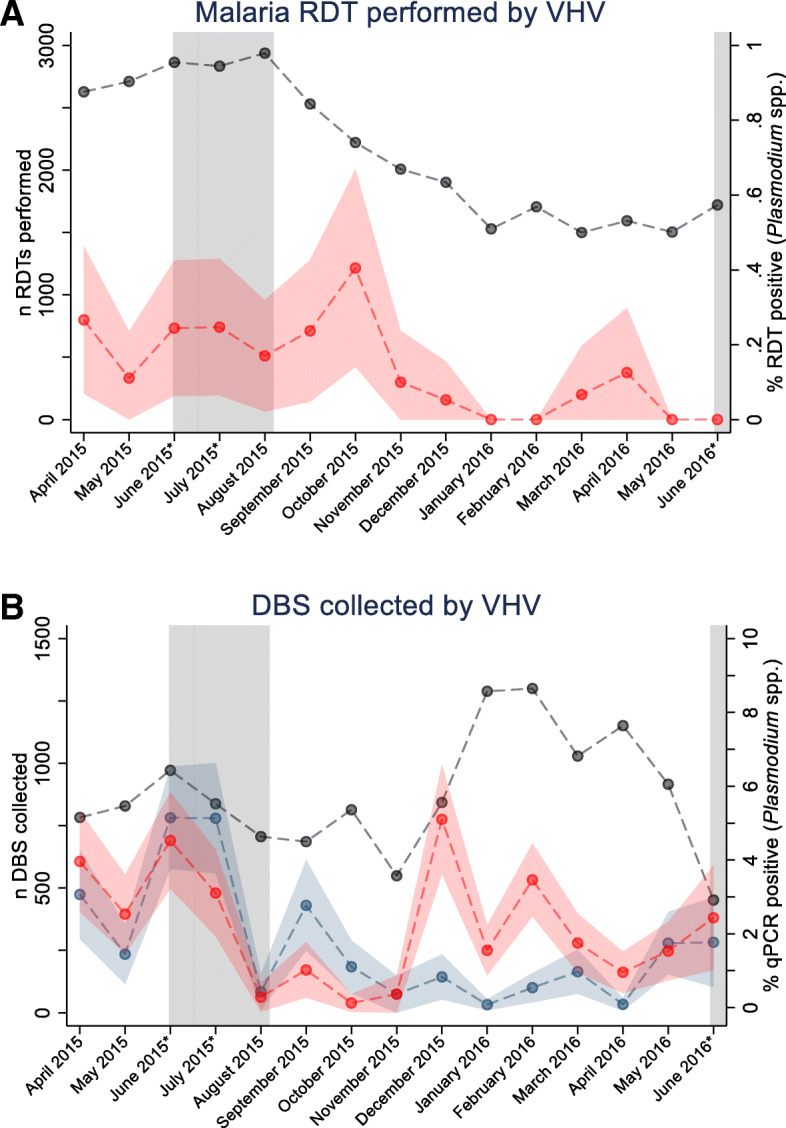
Methods: A total of 114 VHVs were trained to collect dried blood spots from villagers undergoing routine RDTs as part of VHV-led active and passive case detection from April 2015 to June 2016. Samples were subjected to molecular testing (quantitative polymerase chain reaction [qPCR]) to determine Plasmodium falciparum and P. vivax infection and serological testing (against P. falciparum and P. vivax antigens) to determine exposure to P. falciparum and P. vivax.
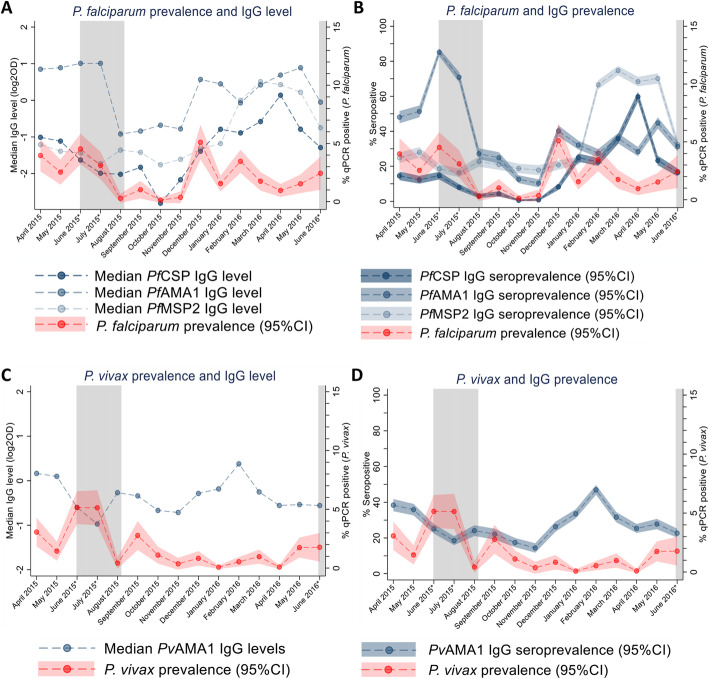
Results: Over 15 months, 114 VHVs performed 32,194 RDTs and collected samples for molecular (n = 13,157) and serological (n = 14,128) testing. The prevalence of molecular-detectable P. falciparum and P. vivax infection was 3.2% compared to the 0.16% prevalence of Plasmodium spp. by RDT, highlighting the large burden of infections undetected by standard surveillance. Peaks in anti-P. falciparum, but not P. vivax, merozoite IgG seroprevalence coincided with seasonal P. falciparum transmission peaks, even in those with no molecularly detectable parasites. At the individual level, antibody seropositivity was associated with reduced odds of contemporaneous P. falciparum (OR for PfCSP 0.51 [95%CI 0.35, 0.76], p = 0.001, PfAMA1 0.70 [95%CI 0.52, 0.93], p = 0.01, and PfMSP2 0.81 [95%CI 0.61, 1.08], p = 0.15), but not P. vivax infection (OR PvAMA1 1.02 [95%CI 0.73, 1.43], p = 0.89) indicating a potential role of immunity in protection against molecular-detectable P. falciparum parasitaemia.
Conclusions: We demonstrated that integration and implementation of sample collection for molecular and serological surveillance into networks of VHV servicing hard-to-reach populations in the GMS is feasible, can capture significant levels of ongoing undetected seasonal malaria transmission and has the potential to supplement current routine RDT testing. Improving malaria surveillance by advancing the integration of molecular and serological techniques, through centralised testing approaches or novel point-of-contact tests, will advance progress, and tracking, towards malaria elimination goals in the GMS.
Keywords: Epidemiology; Immunity; Malaria; Plasmodium; Serosurveillance; Surveillance.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- WHO . Eliminating malaria in the Greater Mekong Subregion. Geneva: World Health Organization; 2016.
-
- WHO . World Malaria Report 2018. Geneva: World Health Organization; 2018.
-
- Zaw MT, Thant M, Hlaing TM, Aung NZ, Thu M, Phumchuea K, Phusri K, Saeseu T, Yorsaeng R, Nguitragool W, Felger I, Kaewkungwal J, Cui L, Sattabongkot J. Asymptomatic and sub-microscopic malaria infection in Kayah State, eastern Myanmar. Malar J. 2017;16(1):138. doi: 10.1186/s12936-017-1789-9. - DOI - PMC - PubMed
-
- Edwards HM, Canavati SE, Rang C, Ly P, Sovannaroth S, Canier L, Khim N, Menard D, Ashton RA, Meek SR, Roca-Feltrer A. Novel cross-border approaches to optimise identification of asymptomatic and artemisinin-resistant Plasmodium infection in mobile populations crossing Cambodian borders. PloS one. 2015;10(9):e0124300. doi: 10.1371/journal.pone.0124300. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
