

Acute Kidney Injury Requiring Dialysis and Incident Dialysis Patient Outcomes in US Outpatient Dialysis Facilities
- PMID: 34045300
- PMCID: PMC8216606
- DOI: 10.2215/CJN.18311120
Acute Kidney Injury Requiring Dialysis and Incident Dialysis Patient Outcomes in US Outpatient Dialysis Facilities
Abstract
Background and objectives: About 30% of patients with AKI may require ongoing dialysis in the outpatient setting after hospital discharge. A 2017 Centers for Medicare & Medicaid Services policy change allows Medicare beneficiaries with AKI requiring dialysis to receive outpatient treatment in dialysis facilities. Outcomes for these patients have not been reported. We compare patient characteristics and mortality among patients with AKI requiring dialysis and patients without AKI requiring incident dialysis.
Design, setting, participants, & measurements: We used a retrospective cohort design with 2017 Medicare claims to follow outpatients with AKI requiring dialysis and patients without AKI requiring incident dialysis up to 365 days. Outcomes are unadjusted and adjusted mortality using Kaplan-Meier estimation for unadjusted survival probability, Poisson regression for monthly mortality, and Cox proportional hazards modeling for adjusted mortality.
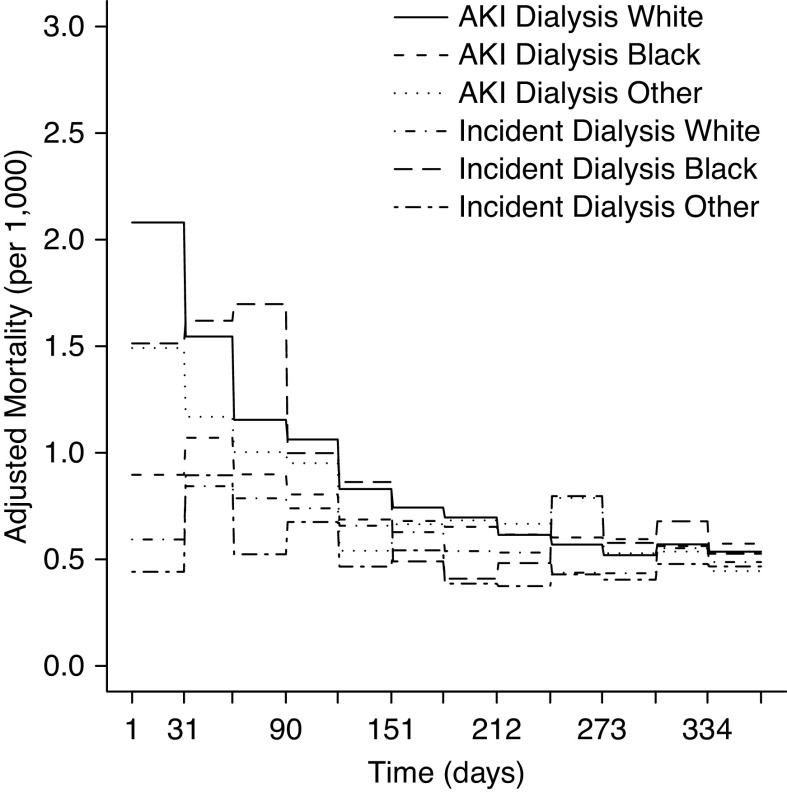
Results: In total, 10,821 of 401,973 (3%) Medicare patients requiring dialysis had at least one AKI claim, and 52,626 patients were Medicare patients without AKI requiring incident dialysis. Patients with AKI requiring dialysis were more likely to be White (76% versus 70%), non-Hispanic (92% versus 87%), and age 60 or older (82% versus 72%) compared with patients without AKI requiring incident dialysis. Unadjusted mortality was markedly higher for patients with AKI requiring dialysis compared with patients without AKI requiring incident dialysis. Adjusted mortality differences between both cohorts persisted through month 4 of the follow-up period (all P=0.01), then, they declined and were no longer statistically significant. Adjusted monthly mortality stratified by Black and other race between patients with AKI requiring dialysis and patients without AKI requiring incident dialysis was lower throughout month 4 (1.5 versus 0.60, 1.20 versus 0.84, 1.00 versus 0.80, and 0.95 versus 0.74; all P<0.001), which persisted through month 7. Overall adjusted mortality risk was 22% higher for patients with AKI requiring dialysis (1.22; 95% confidence interval, 1.17 to 1.27).
Conclusions: In fully adjusted analyses, patients with AKI requiring dialysis had higher early mortality compared with patients without AKI requiring incident dialysis, but these differences declined after several months. Differences were also observed by age, race, and ethnicity within both patient cohorts.
Keywords: ESRD; acute kidney injury; dialysis; mortality risk; outcomes.
Copyright © 2021 by the American Society of Nephrology.
Figures




Comment in
-
Dialyzing Acute Kidney Injury Patients after Hospital Discharge.Clin J Am Soc Nephrol. 2021 Jun;16(6):848-849. doi: 10.2215/CJN.04590421. Epub 2021 Jun 11. Clin J Am Soc Nephrol. 2021. PMID: 34117078 Free PMC article. No abstract available.
References
-
- Wald R, McArthur E, Adhikari NK, Bagshaw SM, Burns KE, Garg AX, Harel Z, Kitchlu A, Mazer CD, Nash DM, Scales DC, Silver SA, Ray JG, Friedrich JO: Changing incidence and outcomes following dialysis-requiring acute kidney injury among critically ill adults: A population-based cohort study. Am J Kidney Dis 65: 870–877, 2015 - PubMed
-
- Rathore AS, Chopra T, Ma JZ, Xin W, Abdel-Rahman EM: Long-term outcomes and associated risk factors of post-hospitalization dialysis-dependent acute kidney injury patients. Nephron 137: 105–112, 2017 - PubMed
-
- Heung M: Outpatient dialysis for acute kidney injury: Progress and pitfalls. Am J Kidney Dis 74: 523–528, 2019 - PubMed
-
- Negi S, Koreeda D, Kobayashi S, Yano T, Tatsuta K, Mima T, Shigematsu T, Ohya M: Acute kidney injury: Epidemiology, outcomes, complications, and therapeutic strategies. Semin Dial 31: 519–527, 2018 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
