

Assessment of cardiovascular risk tools as predictors of cardiovascular disease events in systemic lupus erythematosus
- PMID: 34045359
- PMCID: PMC8162102
- DOI: 10.1136/lupus-2020-000448
Assessment of cardiovascular risk tools as predictors of cardiovascular disease events in systemic lupus erythematosus
Abstract
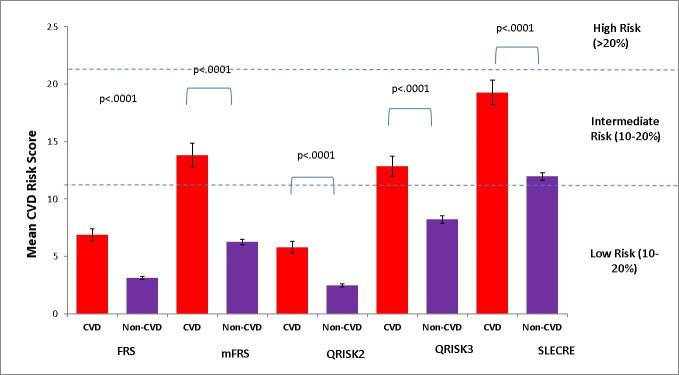
Background: SLE is an independent risk factor for cardiovascular disease (CVD). This study aimed to determine which among QRISK2, QRISK3, Framingham Risk Score (FRS), modified Framingham Risk Score (mFRS) and SLE Cardiovascular Risk Equation (SLECRE) best predicts CVD.
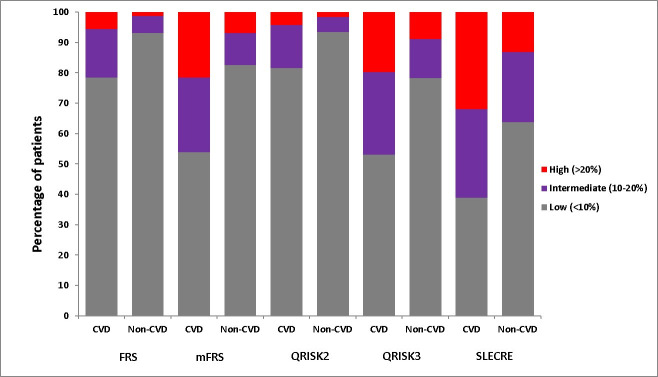
Methods: This is a single-centre analysis on 1887 patients with SLE followed prospectively according to a standard protocol. Tools' scores were evaluated against CVD development at/within 10 years for patients with CVD and without CVD. For patients with CVD, the index date for risk score calculation was chosen as close to 10 years prior to CVD event. For patients without CVD, risk scores were calculated as close to 10 years prior to the most recent clinic appointment. Proportions of low-risk (<10%), intermediate-risk (10%-20%) and high-risk (>20%) patients for developing CVD according to each tool were determined, allowing sensitivity, specificity, positive/negative predictive value and concordance (c) statistics analysis.
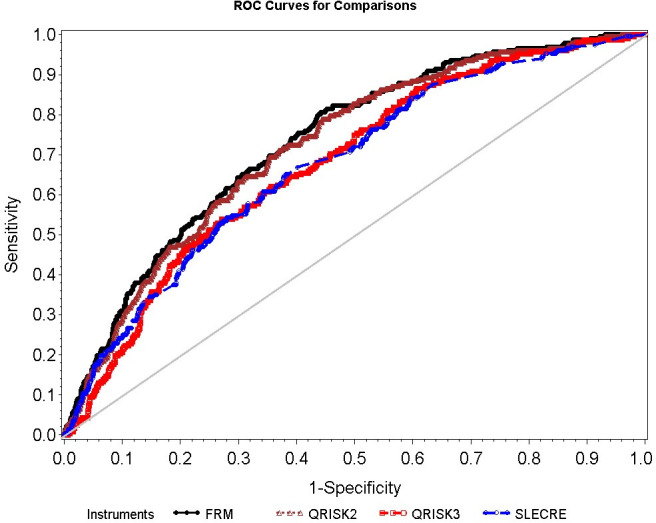
Results: Among 1887 patients, 232 CVD events occurred. QRISK2 and FRS, and QRISK3 and mFRS, performed similarly. SLECRE classified the highest number of patients as intermediate and high risk. Sensitivities and specificities were 19% and 93% for QRISK2, 22% and 93% for FRS, 46% and 83% for mFRS, 47% and 78% for QRISK3, and 61% and 64% for SLECRE. Tools were similar in negative predictive value, ranging from 89% (QRISK2) to 92% (SLECRE). FRS and mFRS had the greatest c-statistics (0.73), while QRISK3 and SLECRE had the lowest (0. 67).
Conclusion: mFRS was superior to FRS and was not outperformed by the QRISK tools. SLECRE had the highest sensitivity but the lowest specificity. mFRS is an SLE-adjusted practical tool with a simple, intuitive scoring system reasonably appropriate for ambulatory settings, with more research needed to develop more accurate CVD risk prediction tools in this population.
Keywords: cardiovascular diseases; inflammation; lupus erythematosus; systemic.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical