

A whole lung in silico model to estimate age dependent particle dosimetry
- PMID: 34045500
- PMCID: PMC8159973
- DOI: 10.1038/s41598-021-90509-8
A whole lung in silico model to estimate age dependent particle dosimetry
Abstract
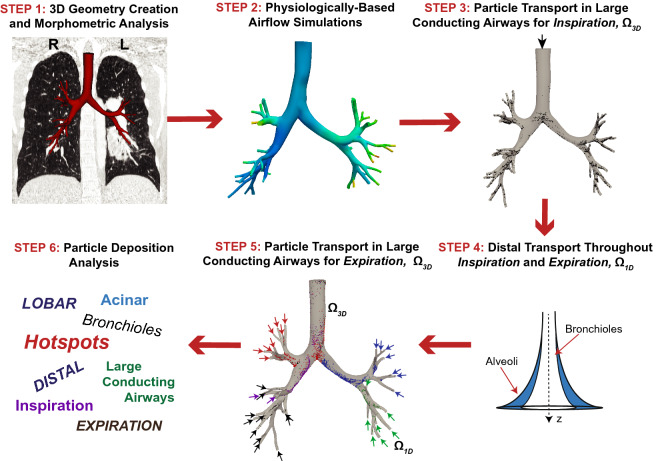
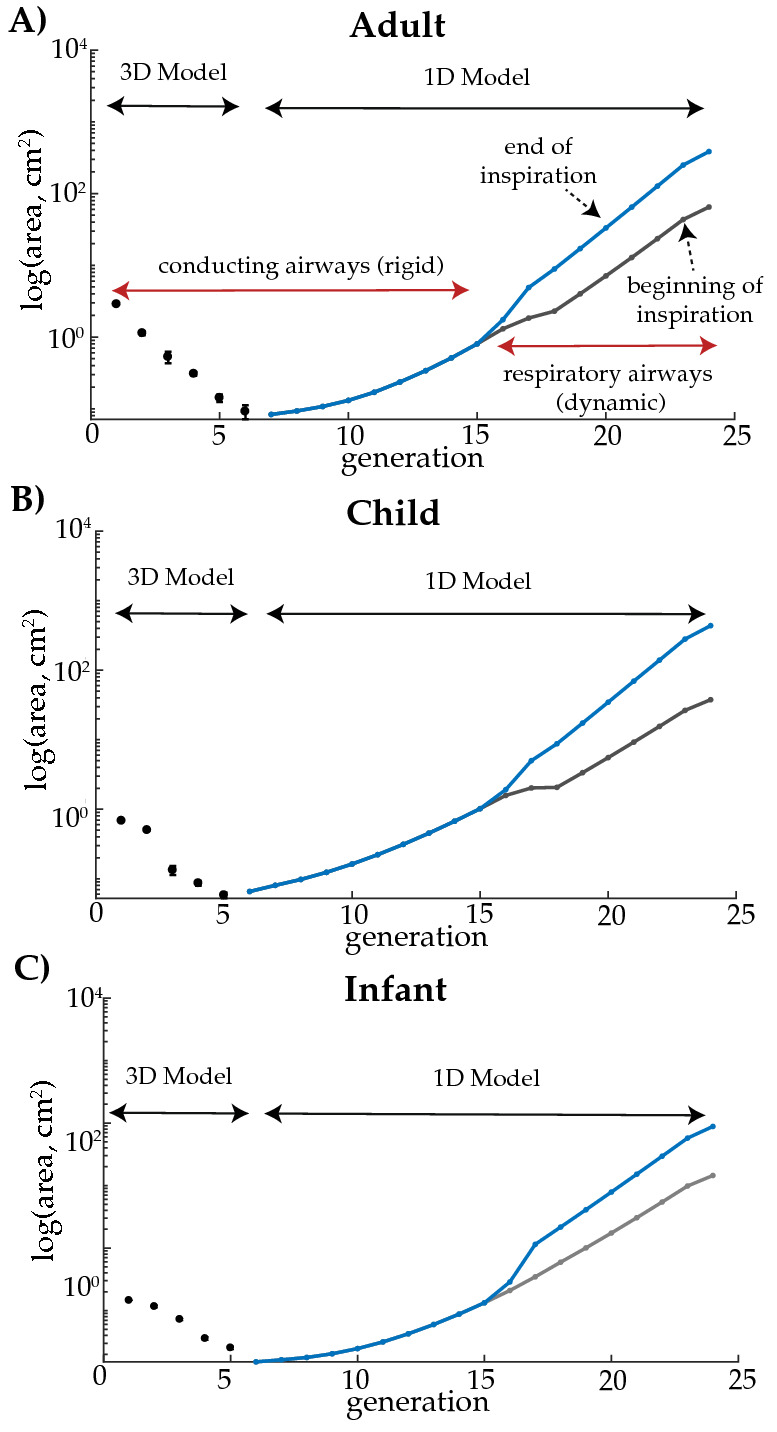
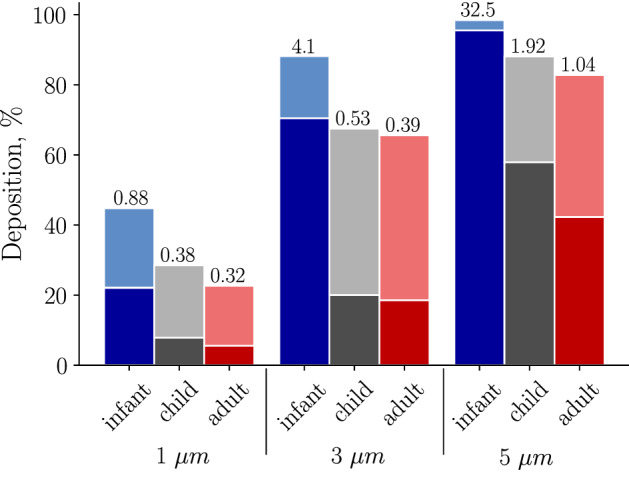
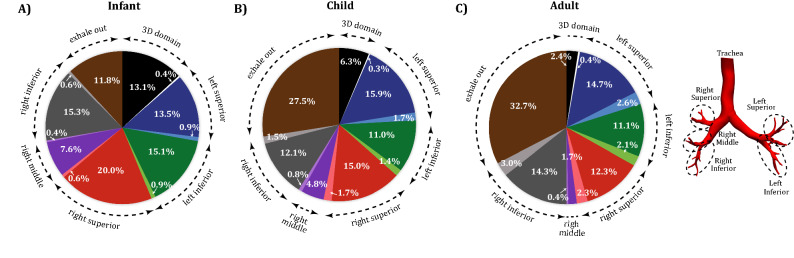
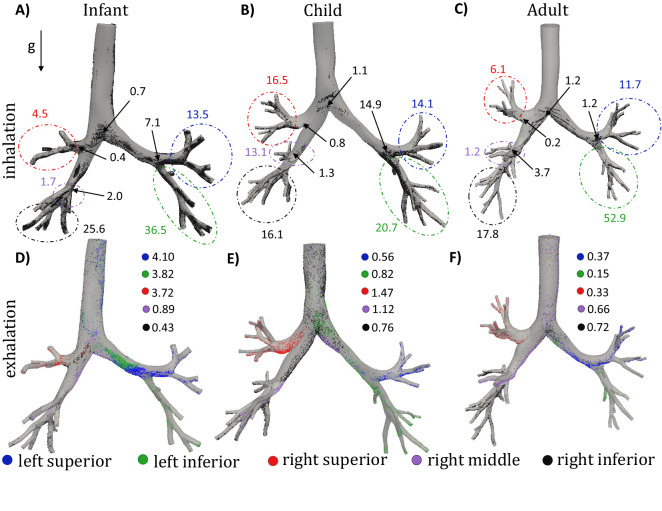
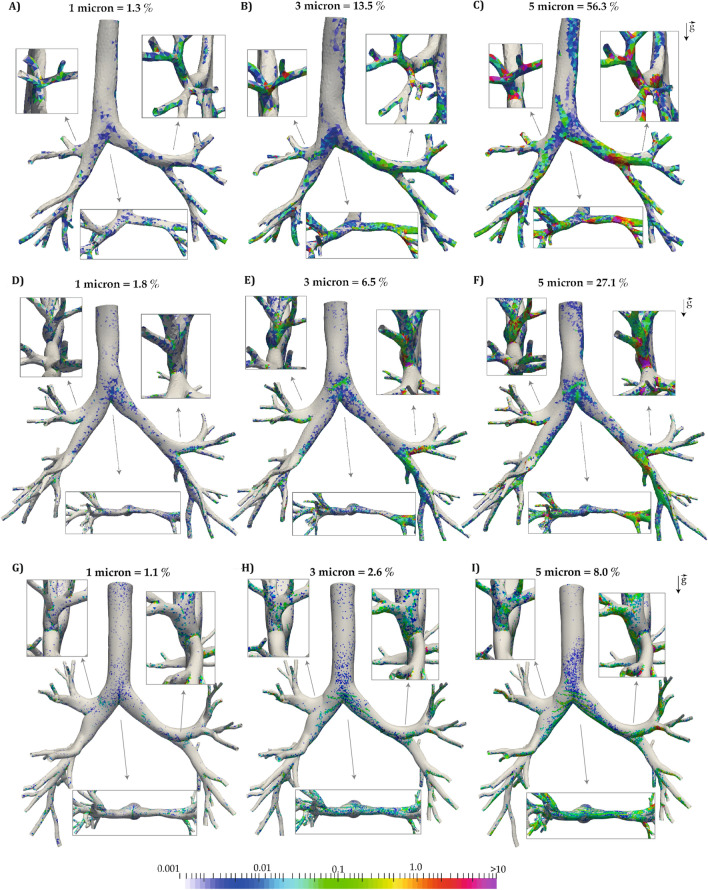
Anatomical and physiological changes alter airflow characteristics and aerosol distribution in the developing lung. Correlation between age and aerosol dosimetry is needed, specifically because youth are more susceptible to medication side effects. In this study, we estimate aerosol dosages (particle diameters of 1, 3, and 5 [Formula: see text]m) in a 3 month-old infant, a 6 year-old child, and a 36 year-old adult by performing whole lung subject-specific particle simulations throughout respiration. For 3 [Formula: see text]m diameter particles we estimate total deposition as 88, 73, and [Formula: see text] and the conducting versus respiratory deposition ratios as 4.0, 0.5, and 0.4 for the infant, child, and adult, respectively. Due to their lower tidal volumes and functional residual capacities the deposited mass is smaller while the tissue concentrations are larger in the infant and child subjects, compared to the adult. Furthermore, we find that dose cannot be predicted by simply scaling by tidal volumes. These results highlight the need for additional clinical and computational studies that investigate the efficiency of treatment, while optimizing dosage levels in order to alleviate side effects, in youth.
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Computational Models of Inhalation Therapy in Early Childhood: Therapeutic Aerosols in the Developing Acinus.J Aerosol Med Pulm Drug Deliv. 2016 Jun;29(3):288-98. doi: 10.1089/jamp.2015.1271. Epub 2016 Feb 23. J Aerosol Med Pulm Drug Deliv. 2016. PMID: 26907858
-
Regional flow and deposition variability in adult female lungs: A numerical simulation pilot study.Clin Biomech (Bristol). 2019 Jun;66:40-49. doi: 10.1016/j.clinbiomech.2017.12.014. Epub 2018 Jan 31. Clin Biomech (Bristol). 2019. PMID: 29395490
-
High-Efficiency Nose-to-Lung Aerosol Delivery in an Infant: Development of a Validated Computational Fluid Dynamics Method.J Aerosol Med Pulm Drug Deliv. 2019 Jun;32(3):132-148. doi: 10.1089/jamp.2018.1490. Epub 2018 Dec 15. J Aerosol Med Pulm Drug Deliv. 2019. PMID: 30556777 Free PMC article.
-
Pediatric in vitro and in silico models of deposition via oral and nasal inhalation.J Aerosol Med Pulm Drug Deliv. 2014 Jun;27(3):149-69. doi: 10.1089/jamp.2013.1075. J Aerosol Med Pulm Drug Deliv. 2014. PMID: 24870701 Review.
-
The utility of hybrid in silico models of airflow and aerosol dosimetry in the lung.J Biomech. 2024 May;168:112126. doi: 10.1016/j.jbiomech.2024.112126. Epub 2024 Apr 27. J Biomech. 2024. PMID: 38718595 Review.
Cited by
-
Recent Developments in Aerosol Pulmonary Drug Delivery: New Technologies, New Cargos, and New Targets.Annu Rev Biomed Eng. 2024 Jul;26(1):307-330. doi: 10.1146/annurev-bioeng-110122-010848. Epub 2024 Jun 20. Annu Rev Biomed Eng. 2024. PMID: 38424089 Free PMC article. Review.
-
Modeling Realistic Geometries in Human Intrathoracic Airways.Diagnostics (Basel). 2024 Sep 7;14(17):1979. doi: 10.3390/diagnostics14171979. Diagnostics (Basel). 2024. PMID: 39272764 Free PMC article. Review.
-
Evaluating the role of sex-related structure-function differences on airway aerosol transport and deposition.J Appl Physiol (1985). 2024 Nov 1;137(5):1285-1300. doi: 10.1152/japplphysiol.00898.2023. Epub 2024 Aug 22. J Appl Physiol (1985). 2024. PMID: 39169840
-
Pulmonary hazards of nanoplastic particles: a study using polystyrene in in vitro models of the alveolar and bronchial epithelium.J Nanobiotechnology. 2025 May 28;23(1):388. doi: 10.1186/s12951-025-03419-6. J Nanobiotechnology. 2025. PMID: 40426130 Free PMC article.
-
Digital twins for chronic lung diseases.Eur Respir Rev. 2024 Dec 18;33(174):240159. doi: 10.1183/16000617.0159-2024. Print 2024 Oct. Eur Respir Rev. 2024. PMID: 39694590 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
