

The importance of the urinary output criterion for the detection and prognostic meaning of AKI
- PMID: 34045582
- PMCID: PMC8159993
- DOI: 10.1038/s41598-021-90646-0
The importance of the urinary output criterion for the detection and prognostic meaning of AKI
Abstract
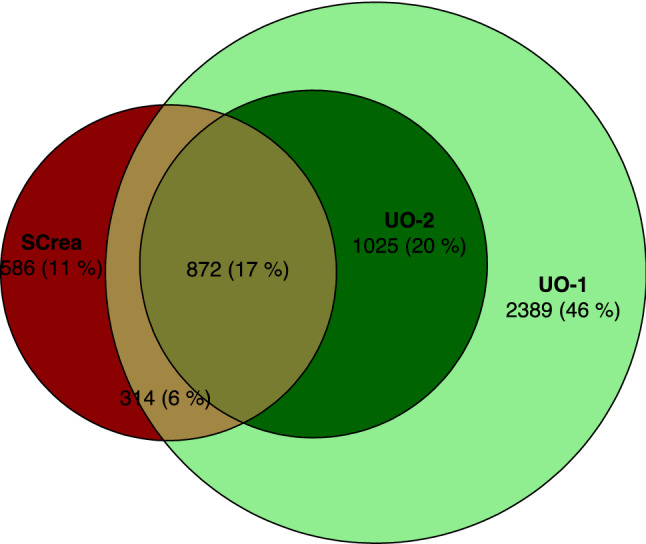
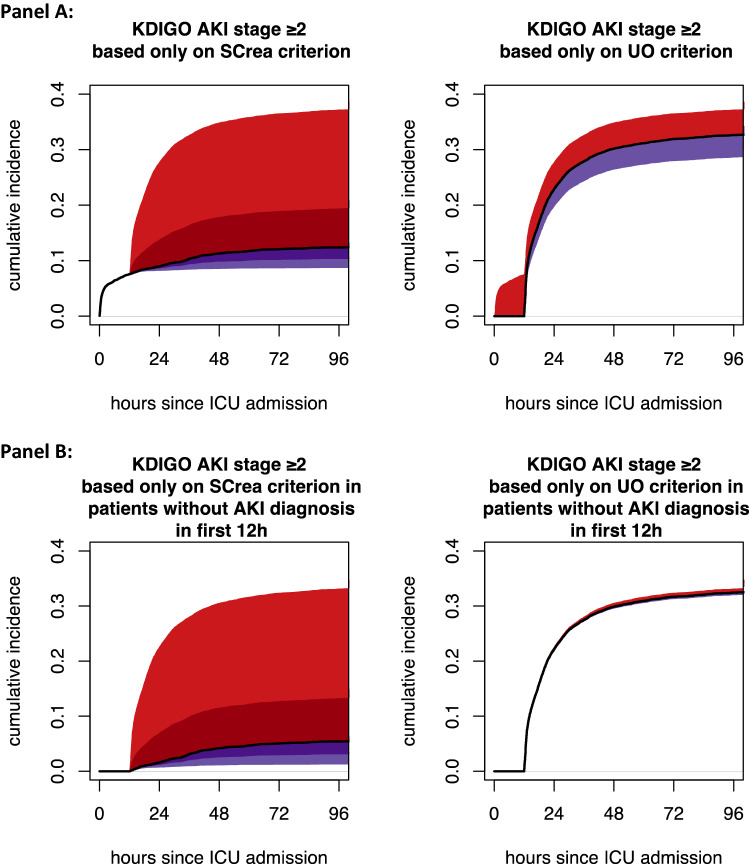
Most reports on AKI claim to use KDIGO guidelines but fail to include the urinary output (UO) criterion in their definition of AKI. We postulated that ignoring UO alters the incidence of AKI, may delay diagnosis of AKI, and leads to underestimation of the association between AKI and ICU mortality. Using routinely collected data of adult patients admitted to an intensive care unit (ICU), we retrospectively classified patients according to whether and when they would be diagnosed with KDIGO AKI stage ≥ 2 based on baseline serum creatinine (Screa) and/or urinary output (UO) criterion. As outcomes, we assessed incidence of AKI and association with ICU mortality. In 13,403 ICU admissions (62.2% male, 60.8 ± 16.8 years, SOFA 7.0 ± 4.1), incidence of KDIGO AKI stage ≥ 2 was 13.2% when based only the SCrea criterion, 34.3% when based only the UO criterion, and 38.7% when based on both criteria. By ignoring the UO criterion, 66% of AKI cases were missed and 13% had a delayed diagnosis. The cause-specific hazard ratios of ICU mortality associated with KDIGO AKI stage ≥ 2 diagnosis based on only the SCrea criterion, only the UO criterion and based on both criteria were 2.11 (95% CI 1.85-2.42), 3.21 (2.79-3.69) and 2.85 (95% CI 2.43-3.34), respectively. Ignoring UO in the diagnosis of KDIGO AKI stage ≥ 2 decreases sensitivity, may lead to delayed diagnosis and results in underestimation of KDIGO AKI stage ≥ 2 associated mortality.
Conflict of interest statement
WVB received travel grants and speaker fees from Fresenius Medical Care, Baxter Healthcare, and Nipro. EH received travel grants and speaker fees from Sopachem and AM Pharma. DB’s institution received grants from Gilead, Astellas, Fisher-Paykel, Baxter, Alexion, and Fresenius Kabi outside the submitted work. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
-
- Bellomo R, Ronco C, Kellum JA, Mehta RL, Palevsky P. Acute renal failure: definition, outcome measures, animal models, fluid therapy and information technology needs: the Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit Care. 2004;8:R204–212. doi: 10.1186/cc2872. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
