

Diagnosis and Treatment of Vulvo-Perineal Endometriosis: A Systematic Review
- PMID: 34046423
- PMCID: PMC8148344
- DOI: 10.3389/fsurg.2021.637180
Diagnosis and Treatment of Vulvo-Perineal Endometriosis: A Systematic Review
Abstract
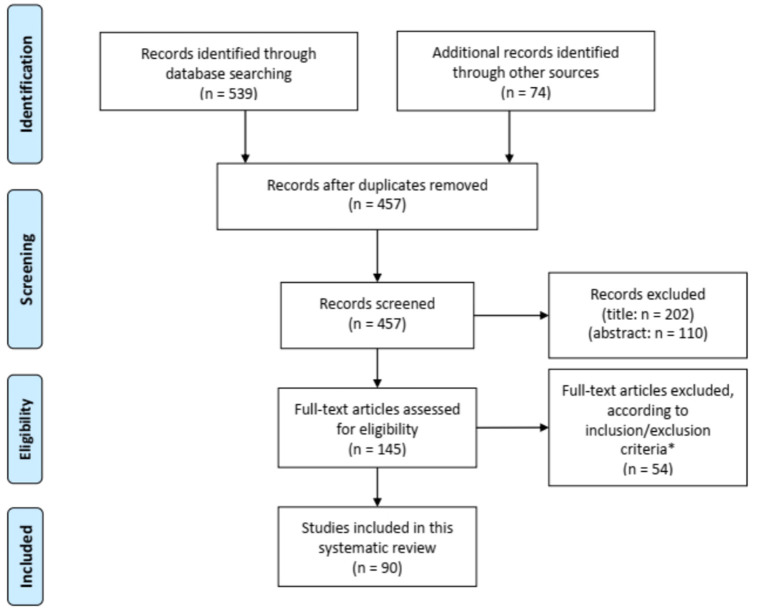
Objective: To describe the available knowledge on vulvo-perineal endometriosis including its diagnosis, clinical management and recurrence rate. Methods: We followed the PRISMA guidelines for Systematic Reviews and our study was prospectively registered with PROSPERO (CRD42020202441). The terms "Endometriosis" and "Perineum" or "Vulva" were used as keywords. Cochrane Library, Medline/Pubmed, Embase and Clinicaltrials.gov were searched. Papers in English, Spanish, Portuguese, French or Italian from inception to July 30, 2020 were considered. Reference lists of included articles and other literature source such as Google Scholar were also manually scrutinized in order to identify other relevant studies. Two independent reviewers screened potentially eligible studies according to inclusion criteria. Results: Out of 539 reports, 90 studies were eligible including a total of 283 patients. Their mean age was 32.7 ± 7.6 years. Two hundred sixty-three (95.3%) presenting with vulvo-perineal endometriosis have undergone either episiotomy, perineal trauma or vaginal injury or surgery. Only 13 patients (4.7%) developed vulvo-vaginal endometriosis spontaneously i.e., without any apparent condition favoring it. The reasons that motivated the patients to take medical advice were vulvo-perineal cyclical pain increasing during menstruations (98.2% of the patients, n = 278). Out of the 281 patients for whom a clinical examination was described, 274 patients (97.5%) showed a vulvo-perineal nodule, mass or swelling while six presented with bluish cutaneous lesions (2.1%) and 1 with bilateral polyps of the labia minora (0.4%). All but one patients underwent surgical excision of their lesions but only 88 patients (28.1%) received additional hormonal therapy. The recurrence rate was 10.2% (29 patients) considering a median follow-up period of 10 months (based on 61 studies). Conclusion: In conclusion, vulvo-perineal endometriosis is a rare entity with approximately 300 cases reported in the literature since 1923. With the available knowledge shown in this systematic review, we encourage all practitioners to think about perineal endometriosis in case of perineal cyclical pain with or without previous perineal damage. Diagnosis should be done with clinical exam, perineal ultrasound and pelvic MRI when available. In case of anal sphincter involvement, perianal ultrasound should be performed. Surgical excision of the lesion should be realized in order to remove the lesion and to confirm the diagnosis histologically. Hormonal treatment could be proposed to attempt to decrease the size of a large lesion before surgery or to avoid recurrence of the lesion. As evidence-based approach to the diagnosis, treatment and recurrence rate of affected patients remains a challenge given its low prevalence, the variations in management found in the articles included and the limited quality of available studies, we suggest that a prospective database on vulvo-perineal endometriosis should be generated to increase knowledge but also awareness among healthcare professionals and optimize patients' care. Systematic Review Registration: https://www.crd.york.ac.uk/prospero/, identifier: CRD42020202441.
Keywords: cyclical pain; endometriosis; episiotomy; extrapelvic endometriosis; perineal nodule; perineal pain; perineum; vulva.
Copyright © 2021 Maillard, Cherif Alami, Squifflet, Luyckx, Jadoul, Thomas and Wyns.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Perineal scar endometriosis involving the anal sphincter. A case report and review of the literature.Ann Ital Chir. 2021 Jan 20;10:S2239253X2103173X. Ann Ital Chir. 2021. PMID: 33480866 Review.
-
Diagnosis and treatment of perineal endometriosis: review of 17 cases.Arch Gynecol Obstet. 2015 Dec;292(6):1295-9. doi: 10.1007/s00404-015-3756-4. Epub 2015 Jun 4. Arch Gynecol Obstet. 2015. PMID: 26041323
-
Abdominal and perineal scar endometriosis: Retrospective study on 40 cases.Eur J Obstet Gynecol Reprod Biol. 2020 Sep;252:225-227. doi: 10.1016/j.ejogrb.2020.06.054. Epub 2020 Jun 26. Eur J Obstet Gynecol Reprod Biol. 2020. PMID: 32623253
-
[Clinical analysis of 30 patients with perineal endometriosis].Zhonghua Yi Xue Za Zhi. 2007 May 8;87(17):1181-3. Zhonghua Yi Xue Za Zhi. 2007. PMID: 17686237 Chinese.
-
Perineal endometriosis with anal sphincter involvement: report of a case.Dis Colon Rectum. 2000 Aug;43(8):1157-60. doi: 10.1007/BF02236565. Dis Colon Rectum. 2000. PMID: 10950016 Review.
Cited by
-
Misdiagnosed as a perianal abscess: case report of perianal endometriosis.J Surg Case Rep. 2024 Aug 30;2024(8):rjae539. doi: 10.1093/jscr/rjae539. eCollection 2024 Aug. J Surg Case Rep. 2024. PMID: 39220168 Free PMC article.
-
Common and uncommon lesions of the vulva and vagina on magnetic resonance imaging: correlations with pathological findings.BJR Open. 2023 Jun 28;5(1):20230002. doi: 10.1259/bjro.20230002. eCollection 2023. BJR Open. 2023. PMID: 37389007 Free PMC article. Review.
-
Episiotomy Scar Endometriosis. Case Presentation.Maedica (Bucur). 2021 Dec;16(4):713-716. doi: 10.26574/maedica.2020.16.4.713. Maedica (Bucur). 2021. PMID: 35261676 Free PMC article.
-
MR imaging of benign vulvar lesions: a pictorial essay.Abdom Radiol (NY). 2025 Feb;50(2):979-994. doi: 10.1007/s00261-024-04524-0. Epub 2024 Aug 24. Abdom Radiol (NY). 2025. PMID: 39180666 Review.
-
Perianal Endometriosis: An Uncommon Site for a Common Problem.Cureus. 2023 Sep 7;15(9):e44840. doi: 10.7759/cureus.44840. eCollection 2023 Sep. Cureus. 2023. PMID: 37809144 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials