

Bilateral posterior scleritis presenting as acute primary angle closure: A case report
- PMID: 34046483
- PMCID: PMC8130077
- DOI: 10.12998/wjcc.v9.i15.3779
Bilateral posterior scleritis presenting as acute primary angle closure: A case report
Abstract
Background: Scleritis is a rare disease and the incidence of bilateral posterior scleritis is even rarer. Unfortunately, misdiagnosis of the latter is common due to its insidious onset, atypical symptoms, and varied manifestations. We report here a case of bilateral posterior scleritis that presented with acute eye pain and intraocular hypertension, and was initially misdiagnosed as acute primary angle closure. Expanding the literature on such cases will not only increase physicians' awareness but also help to improve accurate diagnosis.
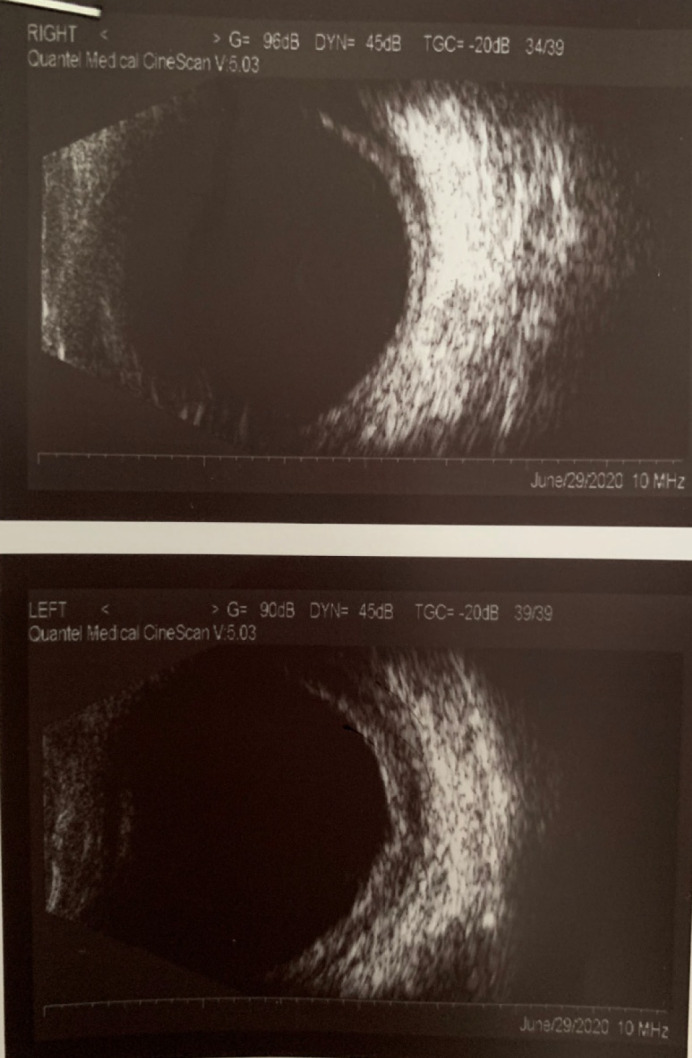
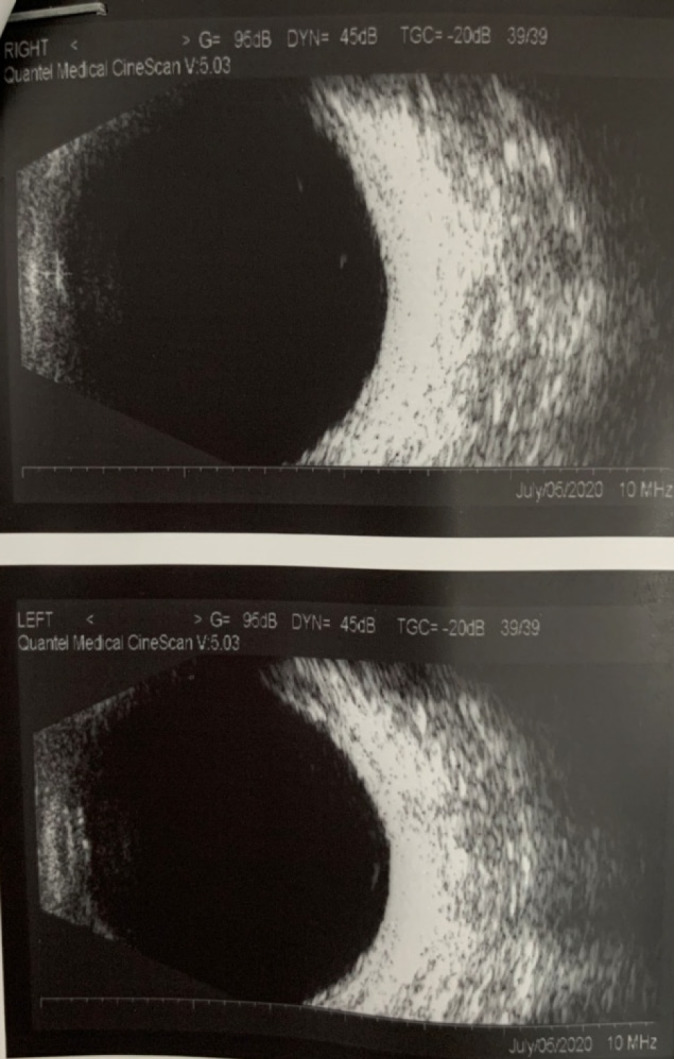
Case summary: A 53-year-old man was referred to our hospital to address a 4-d history of bilateral acute eye pain, headache, and loss of vision, after initial presentation to a local hospital 3 d prior. Our initial examination revealed bilateral cornea edema accompanied by a shallow anterior chamber and visual acuity reduction, with left-eye amblyopia (> 30 years). There was bilateral hypertension (by intraocular pressure: 28 mmHg in right, 34 mmHg in left) and normal fundi. Accordingly, acute primary angle closure was diagnosed. Miotics and ocular hypotensive drugs were prescribed, but the symptoms continued to worsen over the 3-d treatment course. Further imaging examinations (i.e., anterior segment photography and ultrasonography) indicated a diagnosis of bilateral posterior scleritis. Methylprednisolone, topical atropine, and steroid eye drops were prescribed along with intraocular pressure-lowering agents. Subsequent optical coherence tomography (OCT) showed gradual improvements in subretinal fluid under the sensory retina, thickened sclera, and ciliary body detachment.
Conclusion: Bilateral posterior scleritis can lead to secondary acute angle closure. Diagnosis requires ophthalmic accessory examinations (i.e., ultrasound biomicroscopy, B-scan, and OCT).
Keywords: Acute primary angle closure; B-scan; Case report; Differential diagnosis; Optical coherence tomography; Posterior scleritis.
©The Author(s) 2021. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors declare no conflicts of interest.
Figures





Similar articles
-
Monocular posterior scleritis presenting as acute conjunctivitis: A case report.World J Clin Cases. 2020 Oct 26;8(20):5030-5035. doi: 10.12998/wjcc.v8.i20.5030. World J Clin Cases. 2020. PMID: 33195678 Free PMC article.
-
Ciliochoroidal effusion syndrome associated with posterior scleritis.Jpn J Ophthalmol. 2007 Jan-Feb;51(1):49-52. doi: 10.1007/s10384-006-0398-x. Epub 2007 Feb 9. Jpn J Ophthalmol. 2007. PMID: 17295141
-
Posterior Scleritis in a Patient with Psoriasis Masquerading as Acute Angle Closure Glaucoma.Case Rep Ophthalmol. 2022 Sep 30;13(3):717-723. doi: 10.1159/000526714. eCollection 2022 Sep-Dec. Case Rep Ophthalmol. 2022. PMID: 36845449 Free PMC article.
-
Multimodal Imaging of Nodular Posterior Scleritis: Case Report and Review of the Literature.Middle East Afr J Ophthalmol. 2020 Jul 20;27(2):134-138. doi: 10.4103/meajo.MEAJO_115_20. eCollection 2020 Apr-Jun. Middle East Afr J Ophthalmol. 2020. PMID: 32874049 Free PMC article. Review.
-
Acute angle-closure related with choroidal metastasis from lung adenocarcinoma: A case report and literature review.Eur J Ophthalmol. 2024 Mar;34(2):NP33-NP37. doi: 10.1177/11206721231187425. Epub 2023 Jul 9. Eur J Ophthalmol. 2024. PMID: 37424265 Review.
Cited by
-
Unilateral choroidal detachment in an elderly patient with Vogt-Koyanagi-Harada disease: a case report and literature review.Front Immunol. 2025 Feb 27;16:1514306. doi: 10.3389/fimmu.2025.1514306. eCollection 2025. Front Immunol. 2025. PMID: 40083559 Free PMC article. Review.
-
Posterior Scleritis: A Case Report and Literature Review of the Management of the Condition.Cureus. 2024 Jun 2;16(6):e61537. doi: 10.7759/cureus.61537. eCollection 2024 Jun. Cureus. 2024. PMID: 38831917 Free PMC article.
-
A Rare Case of Posterior Scleritis Masquerading as Acute Angle Closure Glaucoma: Highlighting the Diagnostic Value of Multimodal Imaging.Cureus. 2025 Jun 3;17(6):e85282. doi: 10.7759/cureus.85282. eCollection 2025 Jun. Cureus. 2025. PMID: 40612831 Free PMC article.
References
-
- Yang P, Ye Z, Tang J, Du L, Zhou Q, Qi J, Liang L, Wu L, Wang C, Xu M, Tian Y, Kijlstra A. Clinical Features and Complications of Scleritis in Chinese Patients. Ocul Immunol Inflamm. 2018;26:387–396. - PubMed
-
- González-López JJ, Lavric A, Dutta Majumder P, Bansal N, Biswas J, Pavesio C, Agrawal R. Bilateral Posterior Scleritis: Analysis of 18 Cases from a Large Cohort of Posterior Scleritis. Ocul Immunol Inflamm. 2016;24:16–23. - PubMed
-
- Ando Y, Keino H, Nakayama M, Watanabe T, Okada AA. Clinical Features, Treatment, and Visual Outcomes of Japanese Patients with Posterior Scleritis. Ocul Immunol Inflamm. 2020;28:209–216. - PubMed
-
- Gonzalez-Gonzalez LA, Molina-Prat N, Doctor P, Tauber J, Sainz de la Maza M, Foster CS. Clinical features and presentation of posterior scleritis: a report of 31 cases. Ocul Immunol Inflamm. 2014;22:203–207. - PubMed
-
- Erdogan M, Sayin N, YıldızEkinci D, Bayramoglu S. Bilateral Posterior Scleritis Associated with Giant Cell Arteritis: A Case Report. Ocul Immunol Inflamm. 2018;26:1244–1247. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
