

Feasibility of sentinel node navigated surgery in high-risk T1b esophageal adenocarcinoma patients using a hybrid tracer of technetium-99 m and indocyanine green
- PMID: 34046715
- PMCID: PMC8921120
- DOI: 10.1007/s00464-021-08551-6
Feasibility of sentinel node navigated surgery in high-risk T1b esophageal adenocarcinoma patients using a hybrid tracer of technetium-99 m and indocyanine green
Abstract
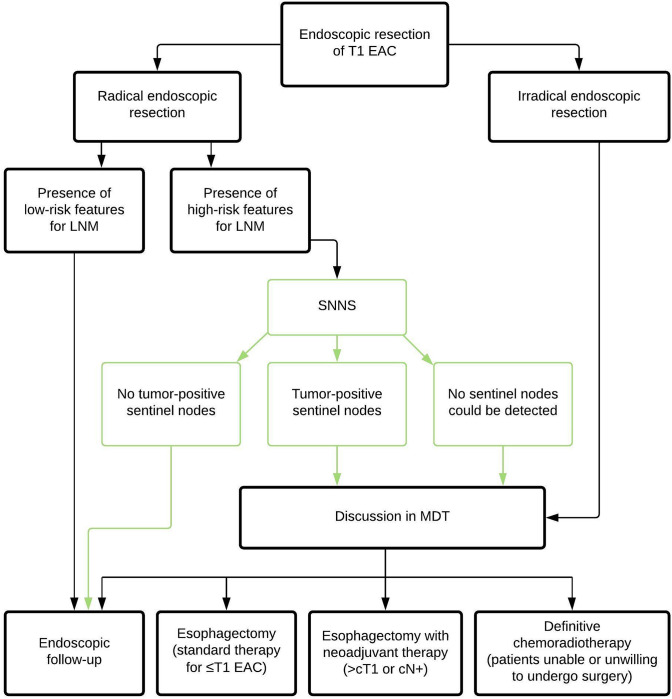
Background: Minimally invasive esophagectomy with two-field lymphadenectomy is standard of care for T1b esophageal adenocarcinoma (EAC) with a high risk of lymph node metastasis. Sentinel node navigation surgery (SNNS) is a well-known concept to tailor the extent of lymphadenectomy. The aim of this study was to evaluate the feasibility and safety of SNNS with a hybrid tracer (technetium-99 m/indocyanine green/nanocolloid) for patients with high-risk T1b EAC.
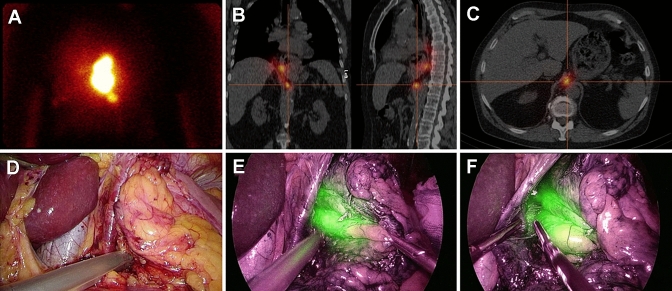
Methods: In this prospective, multicenter pilot study, 5 patients with high-risk T1b EAC were included. The tracer was injected endoscopically around the endoscopic resection scar the day before surgery, followed by preoperative imaging (lymphoscintigraphy/SPECT-CT). During surgery, first the SNs were localized and resected based on preoperative imaging and intraoperative gammaprobe- and fluorescence-based detection, followed by esophagectomy. Primary endpoints were the percentage of patients with detectable SNs, concordance between preoperative and intraoperative SN detection, and the additive value of indocyanine green.
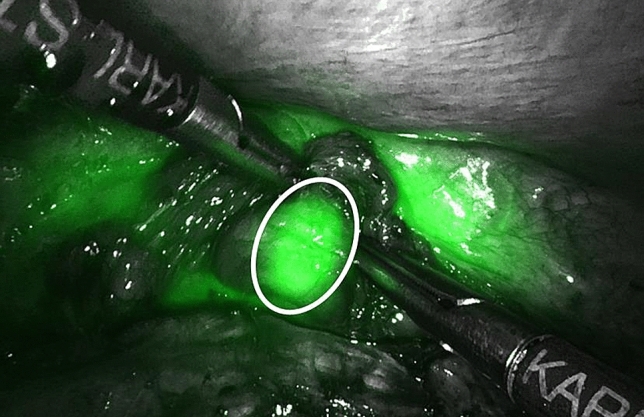
Results: SNs could be identified and resected in all patients (median 3 SNs per patient, range 2-7). There was a high concordance between preoperative and intraoperative SN detection. In 2 patients additional peritumoral SNs were identified with fluorescence-based detection. None of the resected lymph nodes showed signs of (micro)metastases and no nodal metastases were detected in the surgical resection specimen.
Conclusions: SNNS using technetium-99 m/indocyanine green/nanocolloid seems feasible and safe in patients with high-risk T1b EAC. Indocyanine green fluorescence seems to be of additive value for detection of peritumoral SNs. Whether this approach can optimize selection for esophagectomy needs to be studied in future research.
Keywords: Esophageal adenocarcinoma; Esophageal neoplasms; Indocyanine green; Lymph node excision; Sentinel lymph node.
© 2021. The Author(s).
Conflict of interest statement
J.P. Ruurda: proctor Intuitive Surgical. R. van Hillegersberg: proctor Intuitive Surgical and advisory board Medtronic. M.I. van Berge Henegouwen: consultant Medtronic, Johnson & Johnson and Mylan and grants from Olympus and Stryker. A. Overwater, B.L.A.M. Weusten, R.J. Bennink, B. de Keizer, S.L. Meijer, L.A.A. Brosens, R.E. Pouw, J.J.G.H.M. Bergman, and S.S. Gisbertz have no conflicts of interest or financial ties to disclose.
Figures
References
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
