

Neuromyelitis Optica Spectrum Disorder: Clinical Burden and Cost of Relapses and Disease-Related Care in US Clinical Practice
- PMID: 34046846
- PMCID: PMC8571448
- DOI: 10.1007/s40120-021-00253-4
Neuromyelitis Optica Spectrum Disorder: Clinical Burden and Cost of Relapses and Disease-Related Care in US Clinical Practice
Abstract
Introduction: Neuromyelitis optica spectrum disorder (NMOSD) is a rare autoimmune condition characterized by unpredictable relapses that affect the optic nerves and spinal cord, which can lead to blindness, paralysis, and increased mortality rates. Evidence on the clinical and economic burden of NMOSD in the USA is currently lacking.
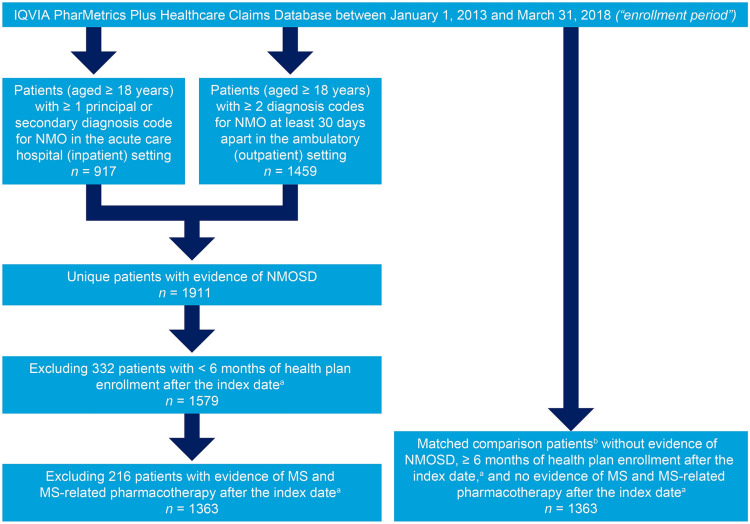
Methods: A retrospective, observational cohort study was conducted using data from the IQVIA PharMetrics Plus Healthcare Claims Database between January 1, 2012 and March 31, 2019. Adults (aged 18 years or more) with evidence of NMOSD and a matched group of comparison patients were identified. Outcomes, including NMOSD relapses, healthcare utilization, and healthcare expenditure (reported in 2018 US dollars), were evaluated during the follow-up period (maximum 6 years). Healthcare utilization and expenditure were assessed overall (all-cause) and during NMOSD relapses.
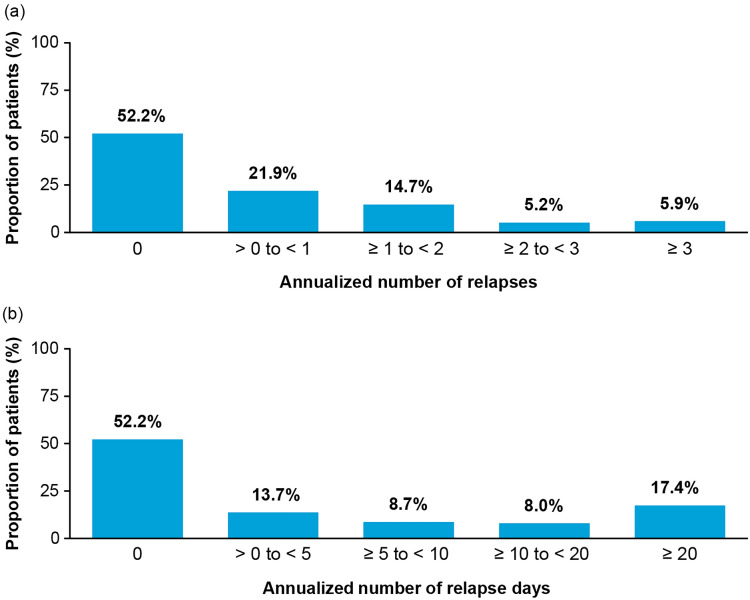
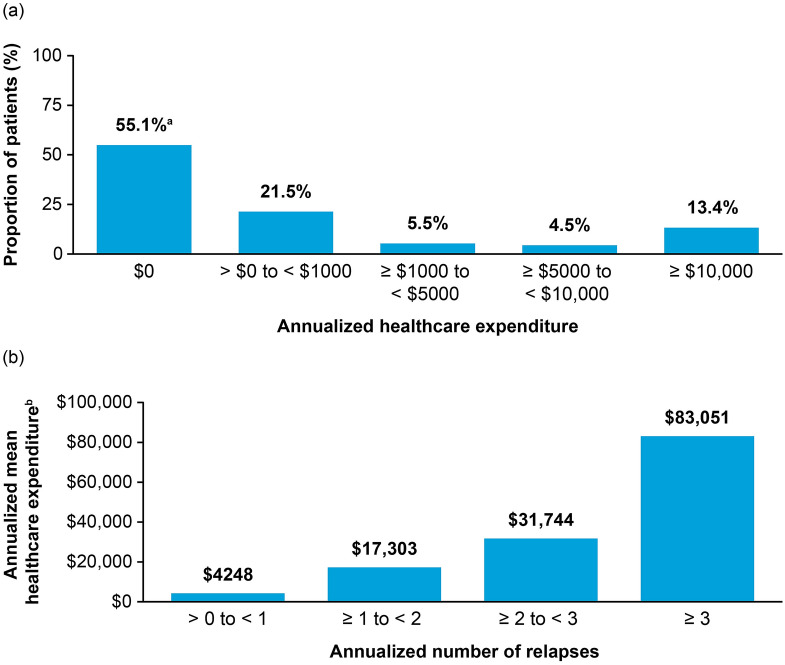
Results: The study included 1363 patients with NMOSD; the mean age was 44.9 years, and 75.3% were female. During the follow-up period (median 2.0 years), 47.7% of patients with NMOSD had one or more relapses, corresponding to an annualized relapse rate of 0.8 (95% confidence interval [CI] 0.7-0.9). When analyzing healthcare expenditure per patient, the mean annualized all-cause healthcare expenditure among patients with NMOSD was $60,599 (95% CI $52,112-66,716) compared with $8912 (95% CI $7084-10,727) among comparison patients, representing a difference of $51,687 (95% CI $43,820-58,664) attributable to NMOSD. The mean annualized total expenditure for NMOSD relapses was $10,070 (95% CI $7726-12,660) per patient, with hospital/inpatient care requiring more expenditure than ambulatory/outpatient care.
Conclusion: Findings of this large, retrospective, observational study indicate that relapses among patients with NMOSD are common in US clinical practice, leading to substantial healthcare utilization and expenditure. Therapies with the highest relapse risk reduction could lead to markedly lower relapse-associated healthcare utilization and clinical burden in patients with NMOSD.
Keywords: Cost of illness; Disease burden; Economic burden; Healthcare costs; Healthcare resource utilization; Neuromyelitis optica; Neuromyelitis optica spectrum disorder; Optic neuritis; Relapses; Transverse myelitis.
Plain language summary
Neuromyelitis optica spectrum disorder (NMOSD) is a severely debilitating neurological disease that affects the nerves in the brain and spinal cord. People who have NMOSD may experience recurrent attacks, or relapses, that can cause blindness and disability. These relapses may lead to hospitalizations, doctor’s office visits, and pharmacy costs that are paid by health insurance plans. Overall, the cost of treating relapses in patients with NMOSD is substantial. Our study analyzed healthcare claims data from the USA. During a median follow-up time of 2.0 years, our study showed that 47.7% of patients with NMOSD experienced one or more relapses, resulting in hospital/inpatient admissions and ambulatory/outpatient treatments. In addition, the average healthcare cost among patients with NMOSD was $60,599 per year compared with $8912 per year for patients without NMOSD. This represents a difference of $51,687 per year, which can be attributed to NMOSD. Among patients with three or more relapses during the follow-up period, the average total healthcare cost was more than $83,000 per patient. Therefore, medicines that prevent relapses could lead to fewer relapse-associated hospitalizations and outpatient treatments for patients with NMOSD.
© 2021. The Author(s).
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
