

Cost-effectiveness of left ventricular assist devices as destination therapy in the United Kingdom
- PMID: 34047072
- PMCID: PMC8318455
- DOI: 10.1002/ehf2.13401
Cost-effectiveness of left ventricular assist devices as destination therapy in the United Kingdom
Abstract
Aims: Continuous-flow left ventricular assist devices (LVADs) as destination therapy (DT) are a recommended treatment by National Institute for Health and Care Excellence England for end-stage heart failure patients ineligible for cardiac transplantation. Despite the fact that DT is frequently used as an LVAD indication across other major European countries and the United States, with consistent improvements in quality-of-life and longevity, National Health Service (NHS) England does not currently fund DT, mainly due to concerns over cost-effectiveness. On the basis of the recently published ENDURANCE Supplemental Trial studying DT patients, we assessed for the first time the cost-effectiveness of DT LVADs compared with medical management (MM) in the NHS England.
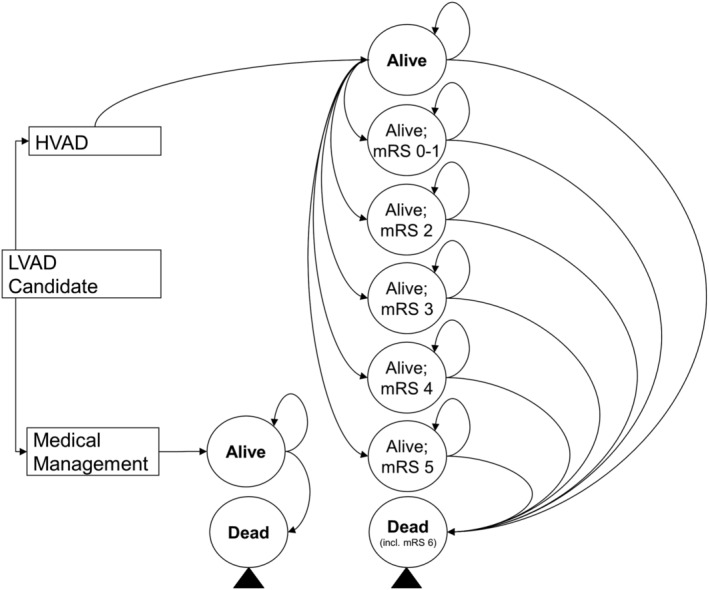
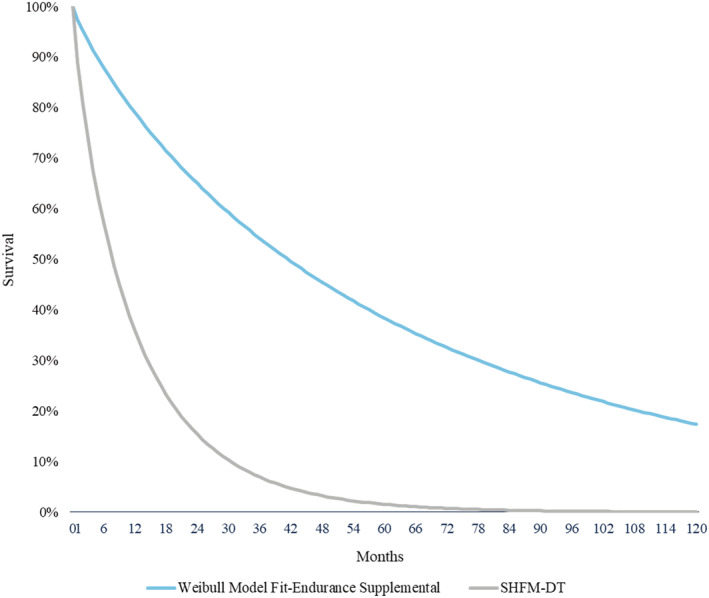
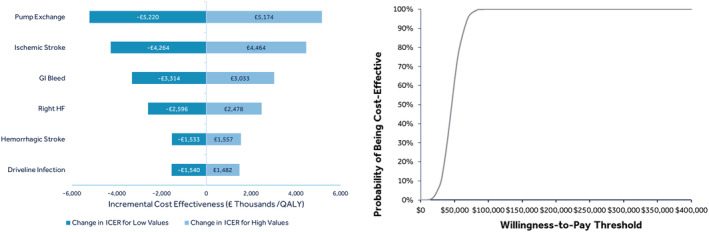
Methods and results: We developed a Markov multiple-state economic model using NHS cost data. LVAD survival and adverse event rates were derived from the ENDURANCE Supplemental Trial. MM survival was based on Seattle Heart Failure Model estimates in the absence of contemporary clinical trials for this population. Incremental cost-effectiveness ratios (ICERs) were calculated over a lifetime horizon. A discount rate of 3.5% per year was applied to costs and benefits. Deterministic ICER was £46 207 per quality-adjusted life year (QALY). Costs and utilities were £204 022 and 3.27 QALYs for the LVAD arm vs. £77 790 and 0.54 QALYs for the MM arm. Sensitivity analyses confirmed robustness of the primary analysis.
Conclusions: The implantation of the HeartWare™ HVAD™ System in patients ineligible for cardiac transplantation as DT is a cost-effective therapy in the NHS England healthcare system under the end-of-life willingness-to-pay threshold of £50 000/QALY, which applies for VAD patients.
Keywords: Cost-effectiveness; Destination therapy; Mechanical circulatory support; Ventricular assist device.
© 2021 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
Professor Schueler is advisor for Medtronic and Leviticus Cardio, and Dr Mahr is a consultant and investigator for Medtronic, Abbott, Abiomed, Syncardia and consultant for Carmat. Dr Silvestry is a consultant for Medtronic, and Abbott. Dr Slaughter is a consultant for Medtronic. Dr Levy is a consultant for Medtronic, and Abbott. Mrs Beckman is a consultant for Medtronic, Abbott, Abiomed and Syncardia. Dr Villinger, Eleni Ismyrloglou, and Stelios Tsintzos are employed by Medtronic. Dr Cheng and Dr Cotts have no relationship with industry.
Figures
Comment in
-
Commentary: Cost-Effectiveness of Left Ventricular Assist Devices as Destination Therapy in the United Kingdom.Front Cardiovasc Med. 2022 Jul 11;9:916588. doi: 10.3389/fcvm.2022.916588. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35898270 Free PMC article. No abstract available.
References
-
- Connolly M, Beattie J, Walker D, Dancy M. End of Life Care in Heart Failure: A Framework for Implementation. London: Quality NICE Improvement; 2014.
-
- Sutcliffe P, Connock M, Pulikottil‐Jacob R, Kandala N, Suri G, Gurung T, Grove A, Shyangdan D, Briscoe S, Maheswaran H. Clinical effectiveness and cost‐effectiveness of second‐and third‐generation left ventricular assist devices as either bridge to transplant or alternative to transplant for adults eligible for heart transplantation: systematic review and cost‐effectiveness model. Health Technol Assess (Winch Eng) 2013; 17: 1–499. - PMC - PubMed
-
- Cleland JG, van Veldhuisen DJ, Ponikowski P. The year in cardiology 2018: heart failure. Eur Heart J 2019; 40: 651–661. - PubMed
-
- McDonagh T, Clark A, Mindham R, de Belder M, Shate A, Ajayi S, Singarayer S. National Heart Failure Audit (NHFA): 2020 Summary Report (2018/19 Data). In: HQIP; 2020.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical