

Induction of labor or expectant management? Birth outcomes for nulliparous individuals choosing midwifery care
- PMID: 34047405
- PMCID: PMC9123647
- DOI: 10.1111/birt.12560
Induction of labor or expectant management? Birth outcomes for nulliparous individuals choosing midwifery care
Abstract
Background: Induction of labor (IOL) has been studied as a strategy to reduce rates of cesarean birth (CB). Midwifery care models are also associated with lower CB rates, even considering that midwives perform fewer IOLs. In this study, we examined childbirth outcomes among individuals undergoing IOL in certified nurse-midwifery (CNM) care as compared to two categories of expectant management (EM).
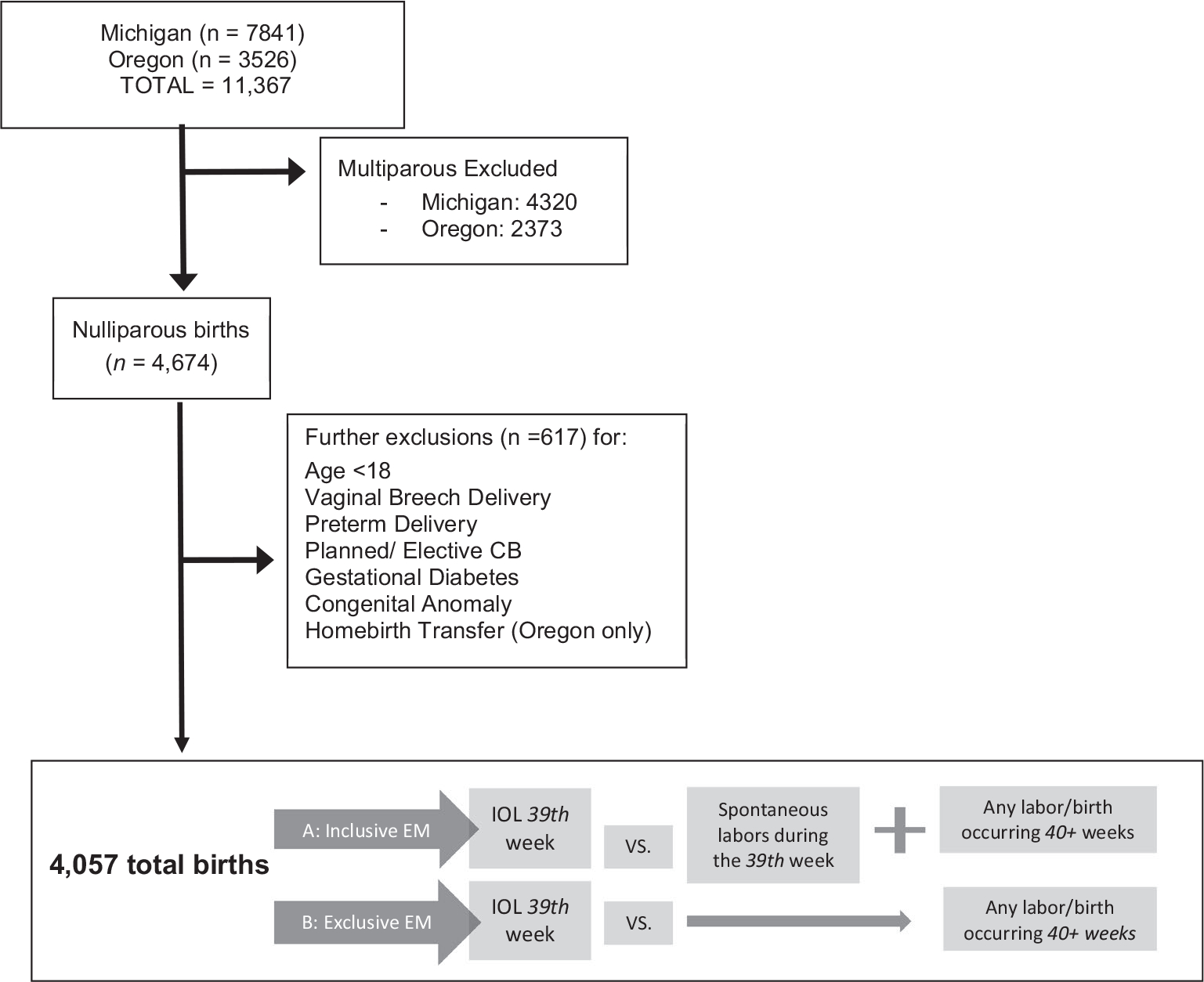
Methods: Data were from two CNM practices in the United States (2007-2018). The sample was limited to term nulliparous, nondiabetic, singleton, vertex pregnancies. Individuals having an IOL in each week of gestation (37th, 38th, etc) were compared with those having EM. Two methods for defining EM were considered as each method when used alone limits interpretation. Inclusive EM included all births starting in the same week as IOL. The exclusive EM group was comprised of all births occurring in the next gestational age week relative to the IOL cases (ie, 39th week IOL versus all births occurring at 40 weeks or later). Adjusted regression models were used to examine differences in CB by IOL versus EM (inclusive or exclusive) at each week of gestation.
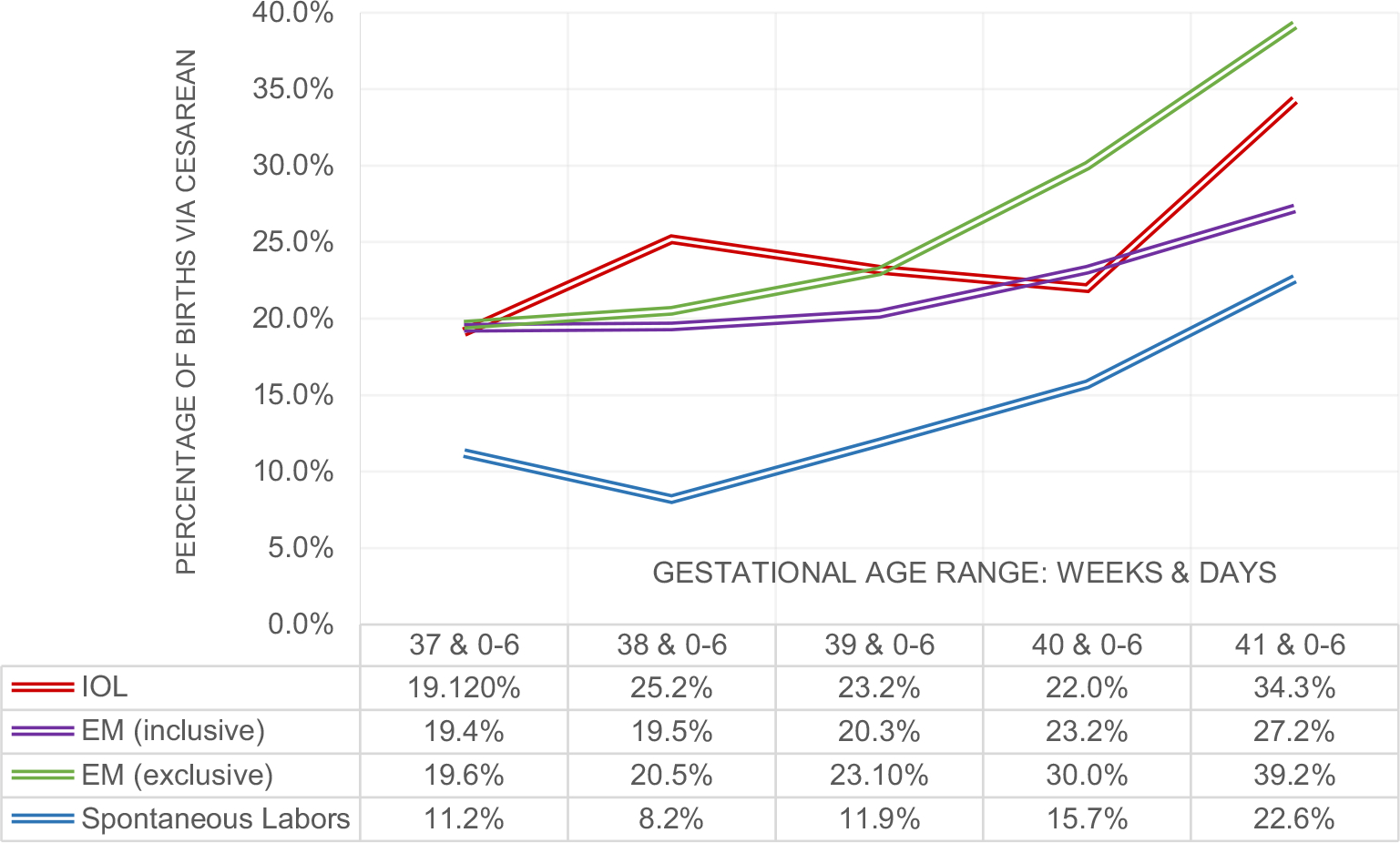
Results: Among 4057 CNM-attended pregnancies, the overall rate of IOL was 28.9% (95% CI 27.5%-30.3%) and CB was 19.4% (95% CI 18.1%-20.6%). Most IOLs involved obstetric indications. CB rates did not differ by IOL versus inclusive EM when performed between 37 and 40 weeks, though post hoc power calculations indicate these comparisons were low-powered. In multivarable models, IOL in the 40th week was associated with lower odds for CB versus exclusive EM definition (ie, births occurring at 41 0/7 weeks or later, OR (95% CI) = 0.57 (0.36-0.90)). This finding is explained by the large increase in CB rates after IOL during the 41st week (34.3%, up from 21.9% in the 40th week). Furthermore, the adjusted odds for CB in the 41st week were 55% higher relative to inclusive EM (all labors 41st week and later), OR (95% CI) = 1.55(1.11-2.15). Neonatal outcomes (aside from macrosomia) did not differ by IOL/EM at any gestational age.
Discussion: Outcomes for nulliparous individuals having IOL or EM in the context of a midwifery model of care include low overall use of CB and low frequency of IOL before 41 weeks. In this model, IOL in the 40th week may lower CB odds, especially in comparison to those who do not have spontaneous labor and later undergo an IOL in the 41st week.
Keywords: cesarean birth; labor induction; midwifery.
© 2021 Wiley Periodicals LLC.
Figures
Similar articles
-
Cesarean delivery after non-medically indicated induction of labor: A population-based study using different definitions of expectant management.Acta Obstet Gynecol Scand. 2021 Feb;100(2):220-228. doi: 10.1111/aogs.13989. Epub 2020 Sep 24. Acta Obstet Gynecol Scand. 2021. PMID: 32880895
-
Maternal and newborn outcomes with elective induction of labor at term.Am J Obstet Gynecol. 2019 Mar;220(3):273.e1-273.e11. doi: 10.1016/j.ajog.2019.01.223. Epub 2019 Feb 17. Am J Obstet Gynecol. 2019. PMID: 30716284
-
Outcomes of Elective Induction of Labor versus Expectant Management among Obese Women at ≥39 Weeks.Am J Perinatol. 2020 Jun;37(7):695-707. doi: 10.1055/s-0039-1688471. Epub 2019 Apr 30. Am J Perinatol. 2020. PMID: 31039597 Free PMC article.
-
Induction of labour at 41 weeks or expectant management until 42 weeks: A systematic review and an individual participant data meta-analysis of randomised trials.PLoS Med. 2020 Dec 8;17(12):e1003436. doi: 10.1371/journal.pmed.1003436. eCollection 2020 Dec. PLoS Med. 2020. PMID: 33290410 Free PMC article.
-
[INDUCTION OF LABOR AT 39 WEEKS OF GESTATION VERSUS EXPECTANT MANAGEMENT].Harefuah. 2019 Dec;158(12):802-806. Harefuah. 2019. PMID: 31823535 Review. Hebrew.
Cited by
-
American College of Nurse-Midwives Clinical Bulletin Number 18: Induction of Labor.J Midwifery Womens Health. 2022 Jan;67(1):140-149. doi: 10.1111/jmwh.13337. J Midwifery Womens Health. 2022. PMID: 35119782 Free PMC article. Review.
-
Maternal Morbidity Predicted by an Intersectional Social Determinants of Health Phenotype: A Secondary Analysis of the NuMoM2b Dataset.Reprod Sci. 2022 Jul;29(7):2013-2029. doi: 10.1007/s43032-022-00913-2. Epub 2022 Mar 21. Reprod Sci. 2022. PMID: 35312992 Free PMC article.
References
-
- Darney BG, Caughey AB. Elective induction of labor symposium: nomenclature, research methodological issues, and outcomes. Clin Obstet Gynecol. 2014;57(2):343–362. - PubMed
-
- Kaimal A, Nicholson J, Cheng Y, Lyell D, Washington A, Caughey A. Induction of labor: Maternal and neonatal complications by gestational age. Am J Obs Gynecol. 2007;197(6):S91.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
