

Symptomatic improvement after mesh removal: a prospective longitudinal study of women with urogynaecological mesh complications
- PMID: 34047446
- PMCID: PMC8497415
- DOI: 10.1111/1471-0528.16778
Symptomatic improvement after mesh removal: a prospective longitudinal study of women with urogynaecological mesh complications
Abstract
Objective: To compare clinical characteristics and outcomes in patients undergoing excision of polypropylene urogynaecological mesh for pain, mesh exposure or both.
Design: Prospective, longitudinal cohort.
Setting: Academic tertiary referral centre.
Population: Women undergoing complete vaginal mesh excision for mesh exposure and/or pain.
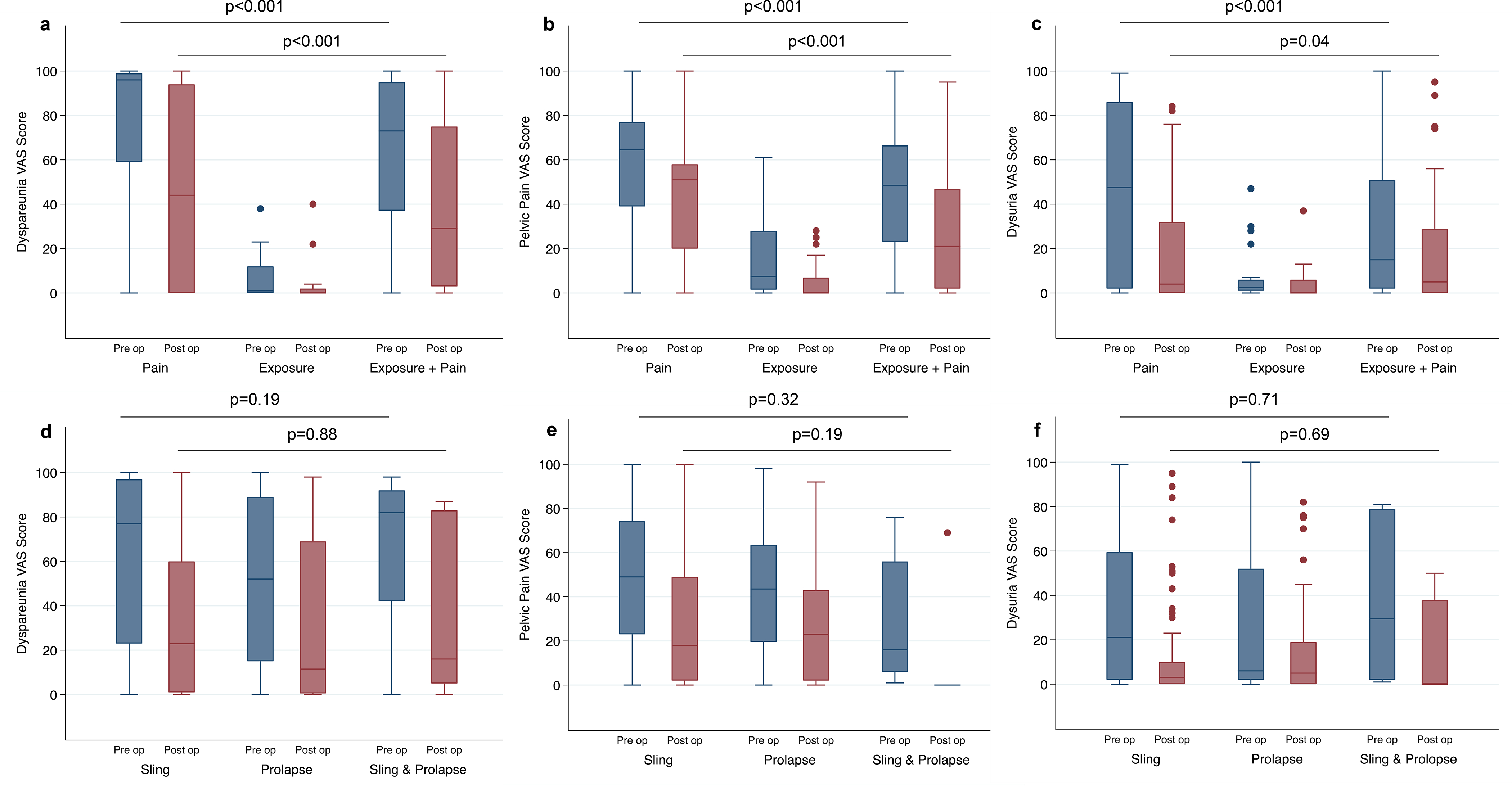
Methods: Clinical and patient-reported outcomes assessing pain (visual analog scale, VAS), bother (Pelvic Floor Distress Inventory, PFDI) and functional impact (Pelvic Functional Impact Questionnaire, PFIQ) were collected at baseline, 6, 12 and 24 months after complete mesh excision. Outcomes were compared by mesh type (sling, prolapse [transvaginal or sacrocolpopexy mesh], both) and complication (pain, exposure, both).
Main outcome measures: 'Much better' or 'Very much better' on Patient Global Impression of Improvement (PGI-I) up to 2 years after removal.
Results: Of 173 women, 48 underwent removal for pain, 27 for exposure and 98 for exposure plus pain. 'Moderate to severe' baseline symptoms were reported by 75%; the most prevalent and severe symptom was dyspareunia. Patients with pain alone were most bothered (PFDI median 234.2, interquartile range 83, P = 0.02) and had the highest functional impact (PFIQ median 181, interquartile range 138, P < 0.001). After excision, only 33.3% of women with pain alone reported 'improved' symptoms (PGI-I), versus 73.9% with exposure, 58.3% with exposure plus pain (P = 0.03) with no differences in PGI-I by mesh type. VAS scores decreased in all groups, but PFDI and PFIQ did not improve in pain patients.
Conclusions: In women experiencing a pain complication after urogynaecological mesh insertion, mesh removal often does not improve symptoms.
Tweetable abstract: Only 33% of women with pain complications have improved symptoms after urogynaecological mesh removal.
Keywords: Complications; mesh removal; patient-reported outcomes; urogynaecological mesh.
© 2021 John Wiley & Sons Ltd.
Figures
Comment in
-
Beware of preoperative pain before implanting a mesh in pelvic floor reconstructive surgery.BJOG. 2021 Nov;128(12):2044-2045. doi: 10.1111/1471-0528.16831. Epub 2021 Jul 28. BJOG. 2021. PMID: 34228887 No abstract available.
Similar articles
-
Diagnosis and management of complications following pelvic organ prolapse surgery using a synthetic mesh: French national guidelines for clinical practice.Eur J Obstet Gynecol Reprod Biol. 2024 Mar;294:170-179. doi: 10.1016/j.ejogrb.2024.01.015. Epub 2024 Jan 17. Eur J Obstet Gynecol Reprod Biol. 2024. PMID: 38280271 Review.
-
A 3-year follow-up after anterior colporrhaphy compared with collagen-coated transvaginal mesh for anterior vaginal wall prolapse: a randomised controlled trial.BJOG. 2016 Jan;123(1):136-42. doi: 10.1111/1471-0528.13628. Epub 2015 Sep 30. BJOG. 2016. PMID: 26420345 Clinical Trial.
-
[Impact of vaginal mesh exposure on quality of life in patients undergoing transvaginal reconstructive pelvic surgery with polypropylene mesh].Zhonghua Fu Chan Ke Za Zhi. 2012 Aug;47(8):608-11. Zhonghua Fu Chan Ke Za Zhi. 2012. PMID: 23141182 Chinese.
-
Laparoscopic complete sacrocolpopexy mesh removal for right-sided gluteal pain and recurrent mesh erosion.Int Urogynecol J. 2020 Feb;31(2):411-413. doi: 10.1007/s00192-019-04088-4. Epub 2019 Sep 3. Int Urogynecol J. 2020. PMID: 31478076
-
Sexual function after pelvic organ prolapse surgery: a systematic review comparing different approaches to pelvic floor repair.Am J Obstet Gynecol. 2021 Nov;225(5):475.e1-475.e19. doi: 10.1016/j.ajog.2021.05.042. Epub 2021 Jun 2. Am J Obstet Gynecol. 2021. PMID: 34087227
Cited by
-
Perioperative Opioid Use in Urogynecologic Mesh Removal.Urogynecology (Phila). 2025 Jan 1;31(1):18-25. doi: 10.1097/SPV.0000000000001527. Urogynecology (Phila). 2025. PMID: 39692525
-
3D Printed Mesh Geometry Modulates Immune Response and Interface Biology in Mouse and Sheep Model: Implications for Pelvic Floor Surgery.Adv Sci (Weinh). 2025 Mar;12(11):e2405004. doi: 10.1002/advs.202405004. Epub 2024 Sep 19. Adv Sci (Weinh). 2025. PMID: 39297316 Free PMC article.
-
Conservative management of intravesical erosion of a synthetic mid-urethral sling for the treatment of stress urinary incontinence, based on patient preference: A case report.Case Rep Womens Health. 2022 Jan 20;33:e00383. doi: 10.1016/j.crwh.2022.e00383. eCollection 2022 Jan. Case Rep Womens Health. 2022. PMID: 35127457 Free PMC article.
-
Biomaterials Interventions for Pelvic Organ Prolapse.JPhys Mater. 2023 Jan;6(1):19-21. Epub 2022 Dec 22. JPhys Mater. 2023. PMID: 36883191 Free PMC article. No abstract available.
References
-
- Nguyen JN, Jakus-Waldman SM, Walter AJ, White T, Menefee SA. Perioperative complications and reoperations after incontinence and prolapse surgeries using prosthetic implants. Obstet Gynecol 2012; 119: 539–546. - PubMed
-
- Kaufmann MR, Scarpero HM, Dmochowski RR. Textbook of Female Urology and Urogynecology, Fourth Edition - Two-Volume Set. 3rd ed. CRC Press: New York, 2010.
-
- Abbott S, Unger CA, Evans JM, Jallad K, Mishra K, Karram MM et al. Evaluation and management of complications from synthetic mesh after pelvic reconstructive surgery: a multicenter study. Am J Obstet Gynecol 2014; 210: 163.e1–8. - PubMed
-
- Unger CA, Abbott S, Evans JM, Jallad K, Mishra K, Karram MM et al. Outcomes following treatment for pelvic floor mesh complications. Int Urogynecol J 2014; 25: 745–749. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
