

Clinicopathologic Features of Oculopharyngodistal Myopathy With LRP12 CGG Repeat Expansions Compared With Other Oculopharyngodistal Myopathy Subtypes
- PMID: 34047774
- PMCID: PMC8164150
- DOI: 10.1001/jamaneurol.2021.1509
Clinicopathologic Features of Oculopharyngodistal Myopathy With LRP12 CGG Repeat Expansions Compared With Other Oculopharyngodistal Myopathy Subtypes
Abstract
Importance: Repeat expansion of CGG in LRP12 has been identified as the causative variation of oculopharyngodistal myopathy (OPDM). However, to our knowledge, the clinicopathologic features of OPDM with CGG repeat expansion in LRP12 (hereafter referred to as OPDM_LRP12) remain unknown.
Objective: To identify and characterize the clinicopathologic features of patients with OPDM_LRP12.
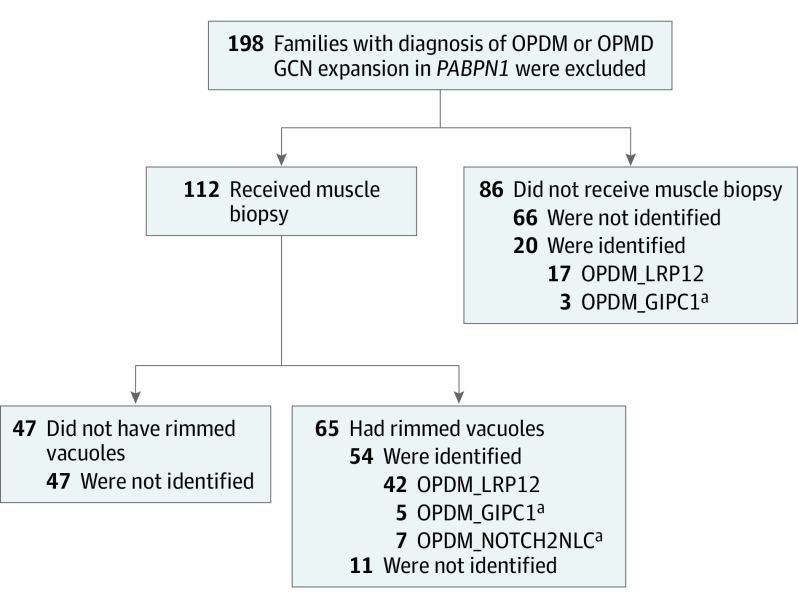
Design, setting, and participants: This case series included 208 patients with a clinical or clinicopathologic diagnosis of oculopharyngeal muscular dystrophy (OPDM) from January 1, 1978, to December 31, 2020. Patients with GCN repeat expansions in PABPN1 were excluded from the study. Repeat expansions of CGG in LRP12 were screened by repeat primed polymerase chain reaction and/or Southern blot.
Main outcomes and measures: Clinical information, muscle imaging data obtained by either computed tomography or magnetic resonance imaging, and muscle pathologic characteristics.
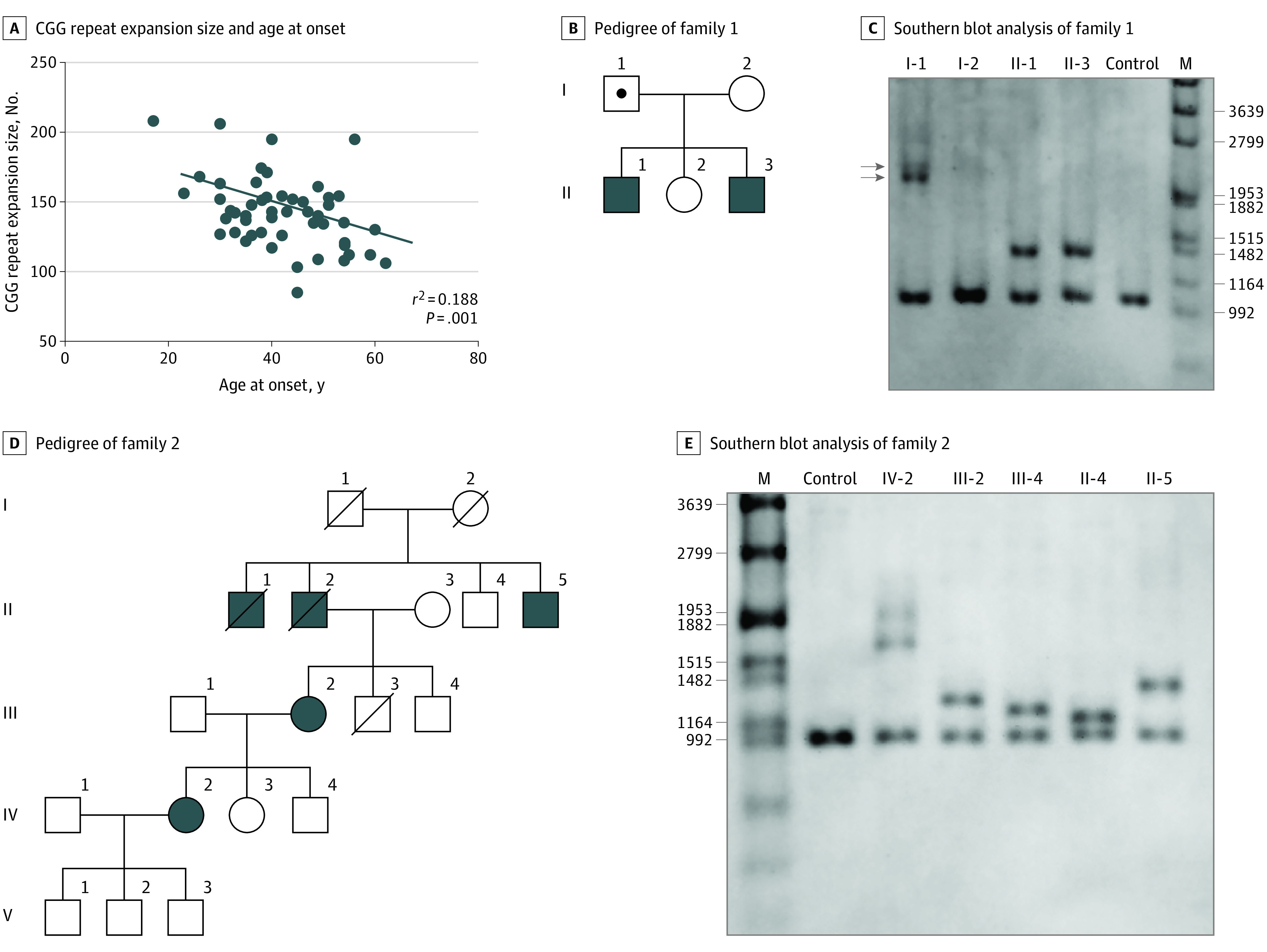
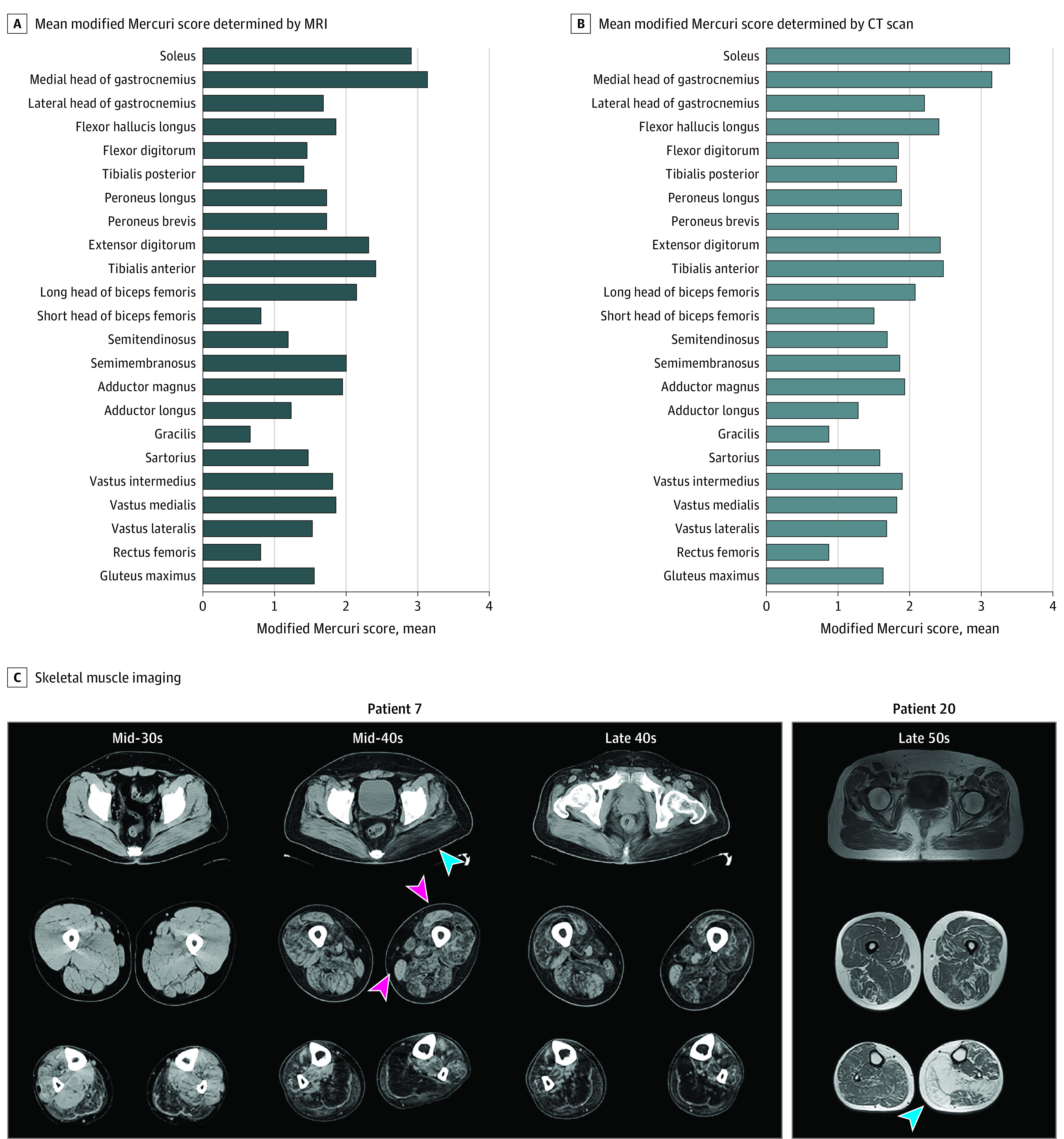
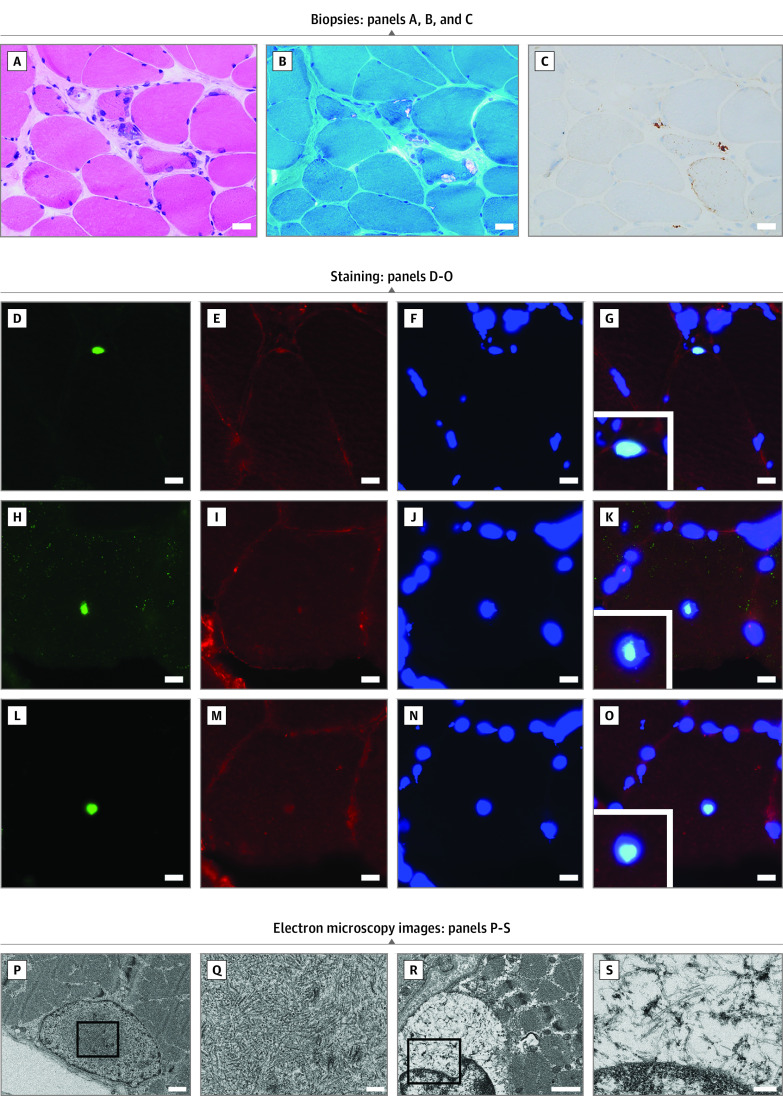
Results: Sixty-five Japanese patients with OPDM (40 men [62%]; mean [SD] age at onset, 41.0 [10.1] years) from 59 families with CGG repeat expansions in LRP12 were identified. This represents the most common OPDM subtype among all patients in Japan with genetically diagnosed OPDM. The expansions ranged from 85 to 289 repeats. A negative correlation was observed between the repeat size and the age at onset (r2 = 0.188, P = .001). The most common initial symptoms were ptosis and muscle weakness, present in 24 patients (37%). Limb muscle weakness was predominantly distal in 53 of 64 patients (83%), but 2 of 64 patients (3%) had predominantly proximal muscle weakness. Ptosis was observed in 62 of 64 patients (97%), and dysphagia or dysarthria was observed in 63 of 64 patients (98%). A total of 21 of 64 patients (33%) had asymmetric muscle weakness. Aspiration pneumonia was seen in 11 of 64 patients (17%), and 5 of 64 patients (8%) required mechanical ventilation. Seven of 64 patients (11%) developed cardiac abnormalities, and 5 of 64 patients (8%) developed neurologic abnormalities. Asymmetric muscle involvement was detected on computed tomography scans in 6 of 27 patients (22%) and on magnetic resonance imaging scans in 4 of 15 patients (27%), with the soleus and the medial head of the gastrocnemius being the worst affected. All 42 muscle biopsy samples showed rimmed vacuoles. Intranuclear tubulofilamentous inclusions were observed in only 1 of 5 patients.
Conclusions and relevance: This study suggests that OPDM_LRP12 is the most frequent OPDM subtype in Japan and is characterized by oculopharyngeal weakness, distal myopathy that especially affects the soleus and gastrocnemius muscles, and rimmed vacuoles in muscle biopsy.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
