

Diffusion-weighted imaging diagnostic algorithm in patients with suspected pleural malignancy
- PMID: 34047851
- PMCID: PMC8589770
- DOI: 10.1007/s00330-021-08013-6
Diffusion-weighted imaging diagnostic algorithm in patients with suspected pleural malignancy
Abstract
Objectives: The purpose of this study was to analyze the diagnostic performance and clinical application of diffusion-weighted imaging (DWI) in patients with suspected pleural malignancy (PM).
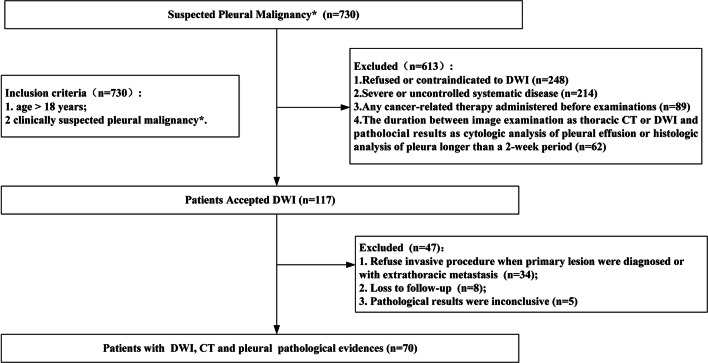
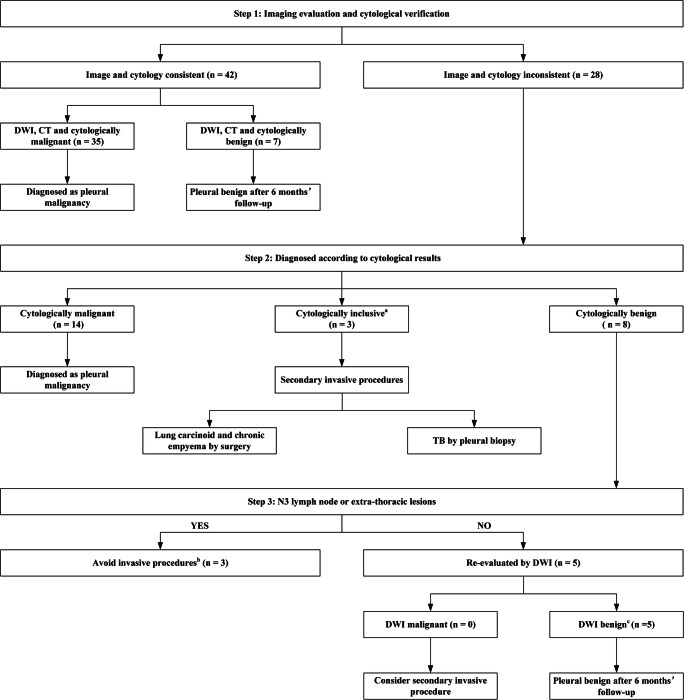
Methods: A retrospective review of patients with suspected PM was performed from March 2014 to August 2018 (NCT02320617). All patients underwent chest DWI and computed tomography (CT) with cytological or histopathological findings as reference standards. The diagnostic performance of DWI and CT was analyzed and compared. A DWI diagnostic algorithm with three sequential steps was established.
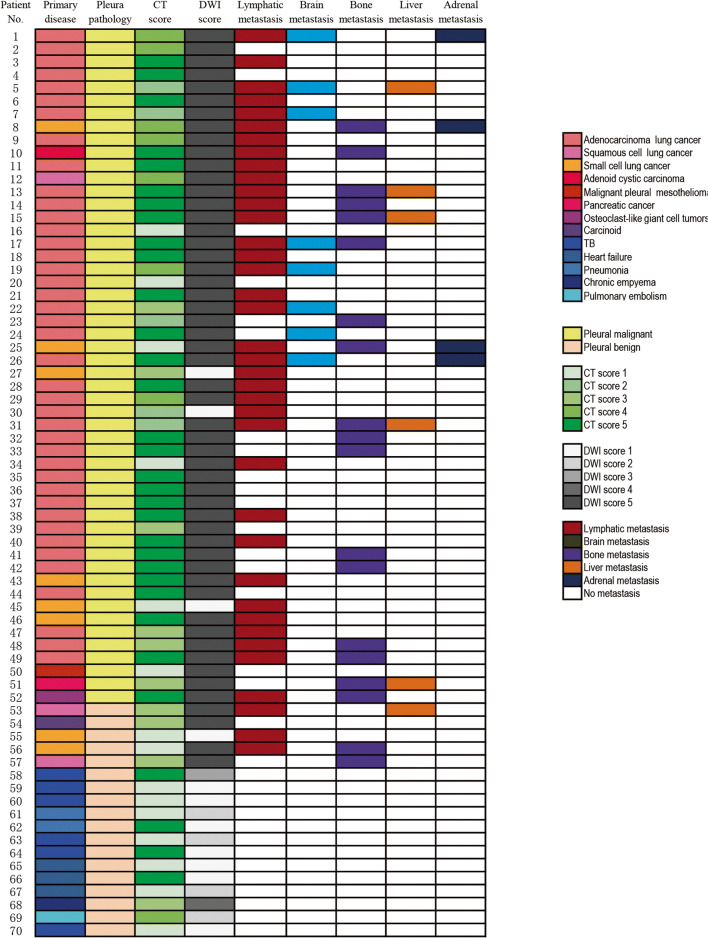
Results: Seventy patients (61.6 ± 13.6 years; 47 males and 23 females) were included. The sensitivity of DWI (94.2%, 49/52) for the diagnosis of PM was significantly higher compared with CT (67.3%, 35/52), with similar specificity (72.2% vs. 72.2%, respectively). The apparent diffusion coefficient of malignant lesions (1.15 ± 0.32 × 10-3 mm2/s) was lower compared with benign lesions (1.46 ± 0.68 × 10-3 mm2/s), but the cutoff value was difficult to define for overlap between groups. Approximately 62.5% (5/8) of invasive procedures were avoided when using the DWI diagnostic algorithm in patients with suspected PM without N3 lymph node or extra-thoracic metastasis.
Conclusion: Including DWI into the diagnostic algorithm of suspected PM can effectively identify malignancy and avoid unnecessary invasive procedures, which may have some potential in clinical application.
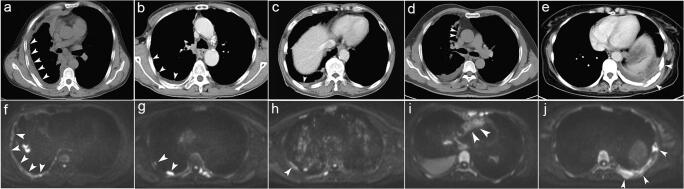
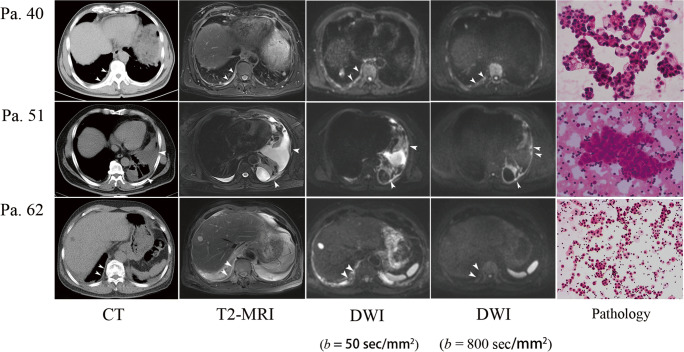
Key points: • Diffusion-weighted imaging can identify pleural malignancy much more efficiently than CT. • A diffusion-weighted imaging diagnostic algorithm helped to avoid unnecessary invasive procedures in patients without N3 lymph node or extra-thoracic lesions. • A hyperintense signal on DWI at a high b value (800 s/mm2) but not at a low b value (50 s/mm2) was a reliable signature of PM.
Keywords: Diffusion magnetic resonance imaging; Pleural neoplasms; Tomography, X-ray computed.
© 2021. The Author(s).
Conflict of interest statement
The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
