

A Roadmap to Cardiac Tissue-Engineered Construct Preservation: Insights from Cells, Tissues, and Organs
- PMID: 34048090
- PMCID: PMC11468174
- DOI: 10.1002/adma.202008517
A Roadmap to Cardiac Tissue-Engineered Construct Preservation: Insights from Cells, Tissues, and Organs
Abstract
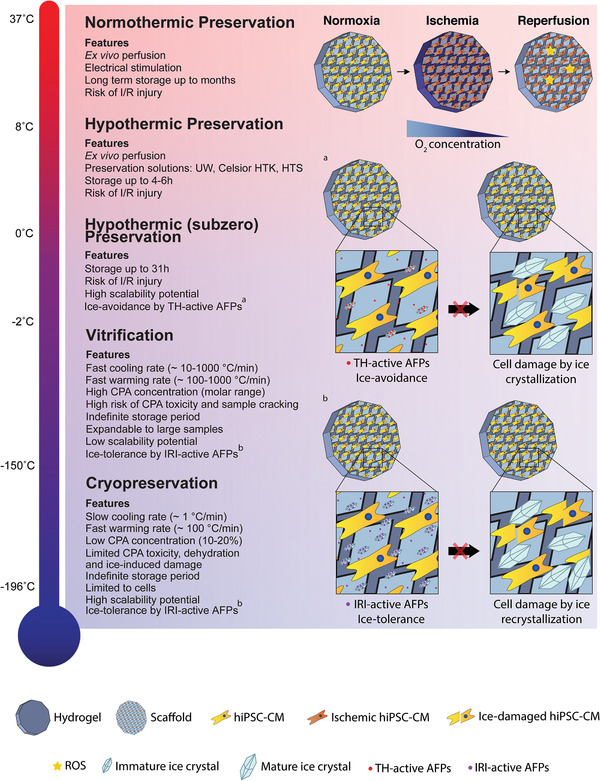
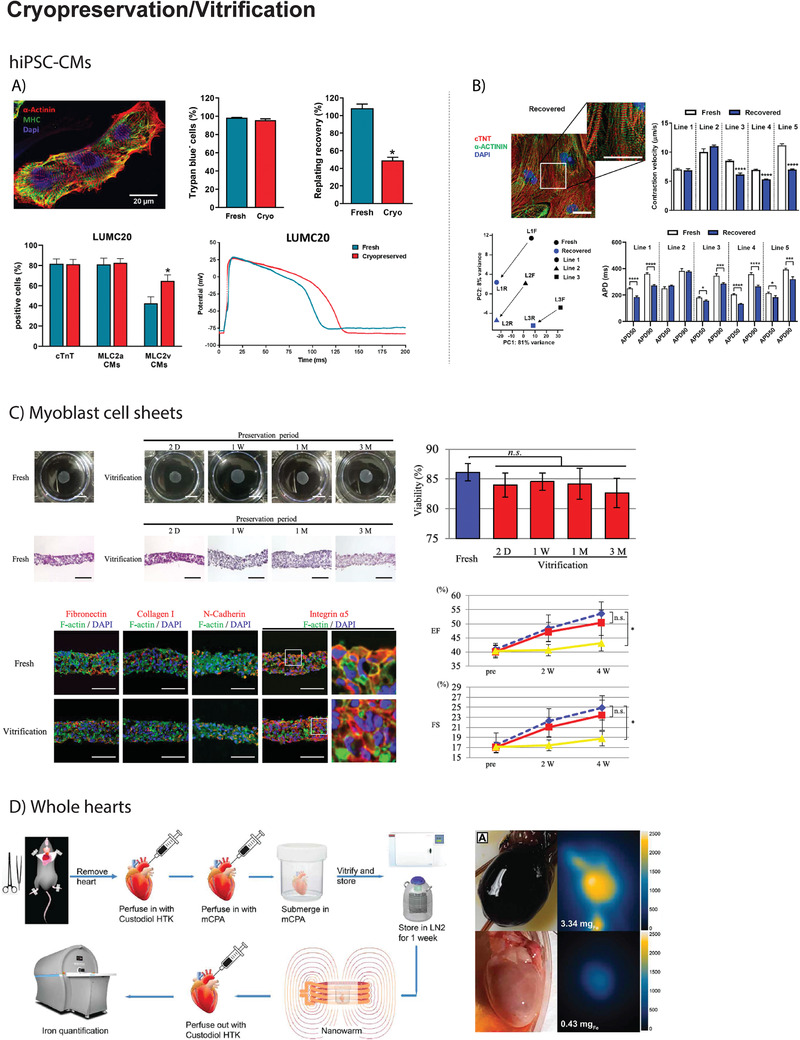
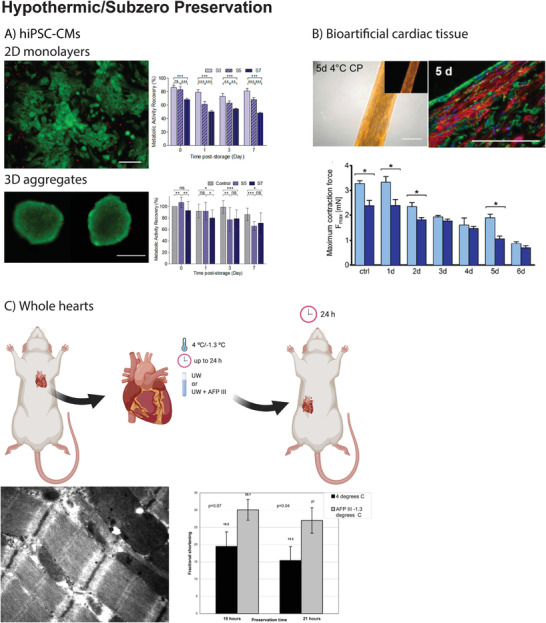
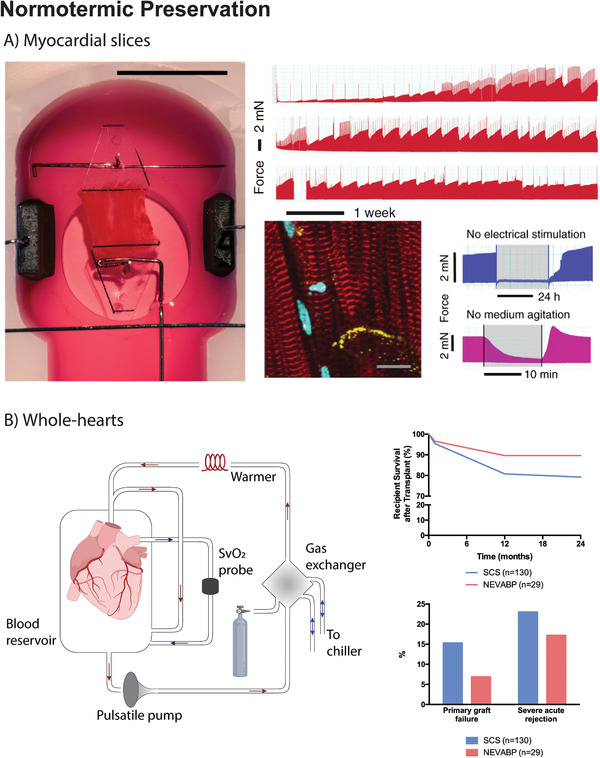
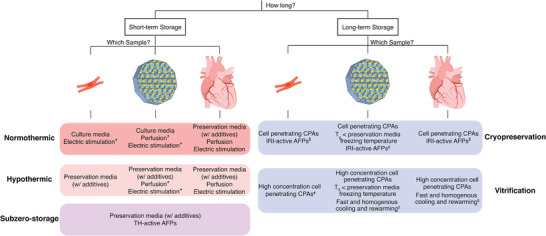
Worldwide, over 26 million patients suffer from heart failure (HF). One strategy aspiring to prevent or even to reverse HF is based on the transplantation of cardiac tissue-engineered (cTE) constructs. These patient-specific constructs aim to closely resemble the native myocardium and, upon implantation on the diseased tissue, support and restore cardiac function, thereby preventing the development of HF. However, cTE constructs off-the-shelf availability in the clinical arena critically depends on the development of efficient preservation methodologies. Short- and long-term preservation of cTE constructs would enable transportation and direct availability. Herein, currently available methods, from normothermic- to hypothermic- to cryopreservation, for the preservation of cardiomyocytes, whole-heart, and regenerative materials are reviewed. A theoretical foundation and recommendations for future research on developing cTE construct specific preservation methods are provided. Current research suggests that vitrification can be a promising procedure to ensure long-term cryopreservation of cTE constructs, despite the need of high doses of cytotoxic cryoprotective agents. Instead, short-term cTE construct preservation can be achieved at normothermic or hypothermic temperatures by administration of protective additives. With further tuning of these promising methods, it is anticipated that cTE construct therapy can be brought one step closer to the patient.
Keywords: antifreeze proteins; cardiac tissue engineering; cryopreservation; cryoprotective agents; heart failure; hypothermic and normothermic preservation; vitrification.
© 2021 The Authors. Advanced Materials published by Wiley-VCH GmbH.
Conflict of interest statement
L.W.v.L. reports consultancy fees to UMCU from Abbott, Medtronic, Vifor, Novartis, and research materials from Roche and Sopachem (all outside of the current work).
Figures
Similar articles
-
Hypothermic and cryogenic preservation of cardiac tissue-engineered constructs.Biomater Sci. 2024 Jul 23;12(15):3866-3881. doi: 10.1039/d3bm01908j. Biomater Sci. 2024. PMID: 38910521 Free PMC article.
-
Cryopreservation of Tissue-Engineered Scaffold-Based Constructs: from Concept to Reality.Stem Cell Rev Rep. 2022 Apr;18(4):1234-1252. doi: 10.1007/s12015-021-10299-4. Epub 2021 Nov 10. Stem Cell Rev Rep. 2022. PMID: 34761366 Review.
-
Curcumin: footprints on cardiac tissue engineering.Expert Opin Biol Ther. 2019 Nov;19(11):1199-1205. doi: 10.1080/14712598.2019.1650912. Epub 2019 Aug 13. Expert Opin Biol Ther. 2019. PMID: 31364892 Review.
-
Nanotechnology-based Cryopreservation of Cell-Scaffold Constructs: A New Breakthrough to Clinical Application.Cryo Letters. 2016 Nov/Dec;37(6):381-387. Cryo Letters. 2016. PMID: 28072423 Review.
-
Development and Application of Cryoprotectants.Adv Exp Med Biol. 2018;1081:339-354. doi: 10.1007/978-981-13-1244-1_18. Adv Exp Med Biol. 2018. PMID: 30288718 Review.
Cited by
-
Genetic Basis of Dilated Cardiomyopathy in Dogs and Its Potential as a Bidirectional Model.Animals (Basel). 2022 Jun 29;12(13):1679. doi: 10.3390/ani12131679. Animals (Basel). 2022. PMID: 35804579 Free PMC article. Review.
-
Hypothermic and cryogenic preservation of cardiac tissue-engineered constructs.Biomater Sci. 2024 Jul 23;12(15):3866-3881. doi: 10.1039/d3bm01908j. Biomater Sci. 2024. PMID: 38910521 Free PMC article.
-
Opportunities and challenges for the use of human samples in translational cardiovascular research: a scientific statement of the ESC Working Group on Cellular Biology of the Heart, the ESC Working Group on Cardiovascular Surgery, the ESC Council on Basic Cardiovascular Science, the ESC Scientists of Tomorrow, the European Association of Percutaneous Cardiovascular Interventions of the ESC, and the Heart Failure Association of the ESC.Cardiovasc Res. 2025 May 23;121(5):702-729. doi: 10.1093/cvr/cvaf023. Cardiovasc Res. 2025. PMID: 40084813 Review.
-
Living myocardial slices: walking the path towards standardization.Cardiovasc Res. 2025 Jul 8;121(7):1011-1023. doi: 10.1093/cvr/cvaf079. Cardiovasc Res. 2025. PMID: 40354127 Free PMC article. Review.
-
Living myocardial slices retain patient-specific features: Insights into etiology and therapeutic history.JHLT Open. 2025 Jul 14;9:100345. doi: 10.1016/j.jhlto.2025.100345. eCollection 2025 Aug. JHLT Open. 2025. PMID: 40799359 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
- 2019T056/The Netherlands Heart Foundation
- Technische Universiteit Eindhoven
- ERC-2014-StG/European Union
- 635928/European Union
- 712.016.002/Dutch Science Foundation
- 725229/European Union: ERC-2016-CoG
- 024.003.013/Netherlands Organization for Scientific Research
- 801540/Horizon 2020 Marie Skłodowska-Curie Actions
- the Leducq Fondation grant to the Cure-PLaN network
- H2020/BRAV∃
- ID:874827/BRAV∃
- PTDC/BTMSAL/32566/2017/Fundação para a Ciência e a Tecnologia
- UIDB/04462/2020/iNOVA4Health
- UIDP/04462/2020/iNOVA4Health
- FCT/Ministério da Ciência, Tecnologia e Ensino Superior
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
