

Effectiveness of early versus delayed rehabilitation following rotator cuff repair: Systematic review and meta-analyses
- PMID: 34048450
- PMCID: PMC8162656
- DOI: 10.1371/journal.pone.0252137
Effectiveness of early versus delayed rehabilitation following rotator cuff repair: Systematic review and meta-analyses
Abstract
Objective: To investigate the effectiveness of early rehabilitation compared with delayed/standard rehabilitation after rotator cuff repair for pain, function, range of movement, strength, and repair integrity.
Design: Systematic review and meta-analyses.
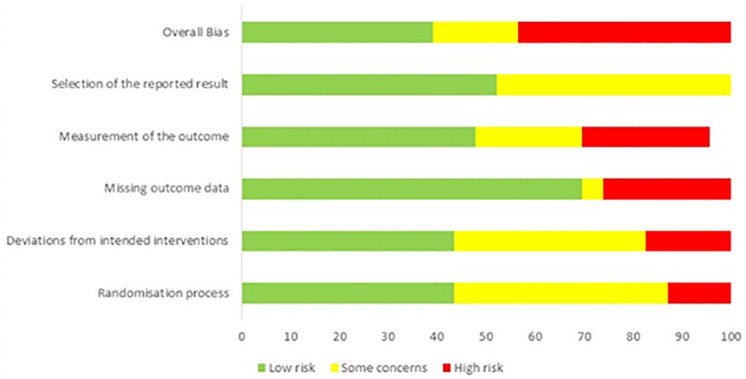
Methods: We searched databases and included randomised controlled trials (RCTs) comparing early with delayed/standard rehabilitation for patients undergoing rotator cuff repair surgery. We assessed risk of bias of the RCTs using the Cochrane RoB 2 tool.
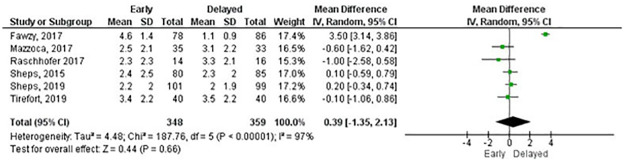
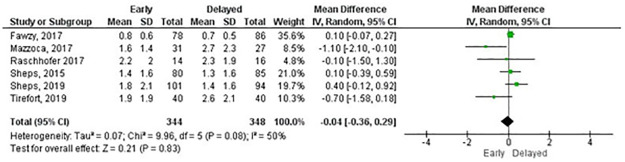
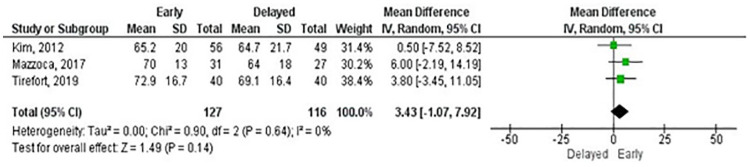
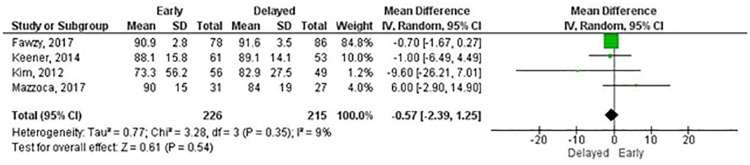
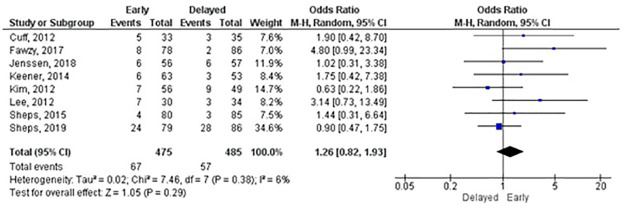
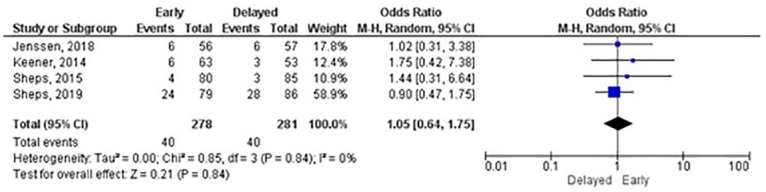
Results: Twenty RCTs, with 1841 patients, were included. The majority of the RCTs were of high or unclear risk of overall bias. We found substantial variations in the rehabilitation programmes, time in the sling and timing of exercise progression. We found no statistically significant differences for pain and function at any follow-up except for the outcome measure Single Assessment Numeric Evaluation at six months (MD: 6.54; 95%CI: 2.24-10.84) in favour of early rehabilitation. We found statistically significant differences in favour of early rehabilitation for shoulder flexion at six weeks (MD: 7.36; 95%CI: 2.66-12.06), three (MD: 8.45; 95%CI: 3.43-13.47) and six months (MD: 3.57; 95%CI: 0.81-6.32) and one year (MD: 1.42; 95%CI: 0.21-2.64) and similar differences for other planes of movement. In terms of repair integrity, early mobilisation does not seem to increase the risk of re-tears (OR:1.05; 95%CI: 0.64-1.75).
Discussion: Current approaches to early mobilisation, based largely on early introduction of passive movement, did not demonstrate significant differences in most clinical outcomes, although we found statistically significant differences in favour of early rehabilitation for range of movement. Importantly, there were no differences in repair integrity between early and delayed/standard rehabilitation. Most rehabilitation programmes did not consider early active movement as soon as the patient feels able. With ongoing variation in rehabilitation protocols there remains a need for large high quality RCT to inform the optimal approach to rehabilitation after rotator cuff repair surgery.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- Littlewood C, May S, Walters S. Epidemiology of rotator cuff tendinopathy: a systematic review. Shoulder & Elbow. 2013;5(4):256–65.
-
- HES. Hospital Episode Statistics, Hospital Admitted Patient Care Activity 2018–19 [Internet] https://digital.nhs.uk/data-and-information/publications/statistical/hos...
-
- Funk L. Arthroscopic shoulder surgery has progressed, has the rehabilitation? International Musculoskeletal Medicine. 2012;34(4):141–5.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
