

Focused ultrasound of the caudal vena cava in dogs with cavitary effusions or congestive heart failure: A prospective, observational study
- PMID: 34048483
- PMCID: PMC8162640
- DOI: 10.1371/journal.pone.0252544
Focused ultrasound of the caudal vena cava in dogs with cavitary effusions or congestive heart failure: A prospective, observational study
Abstract
Introduction: Ultrasonographic indices of the inferior vena cava are useful for predicting right heart filling pressures in people.
Objectives: To determine whether ultrasonographic indices of caudal vena cava (CVC) differ between dogs with right-sided CHF (R-CHF), left-sided CHF (L-CHF), and noncardiac causes of cavitary effusion (NC).
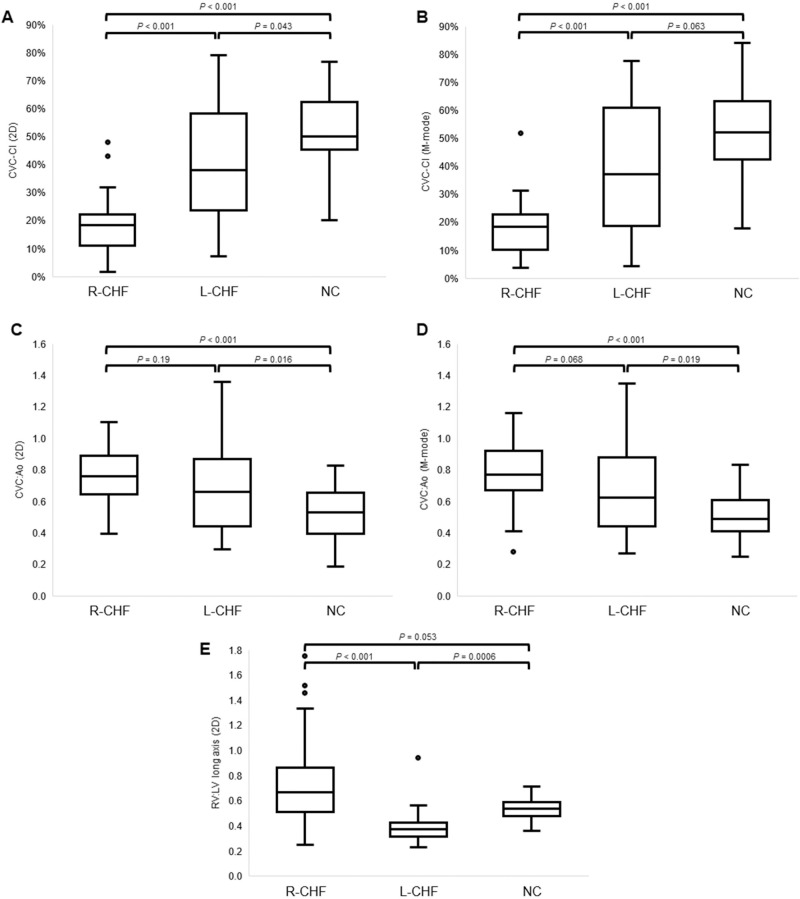
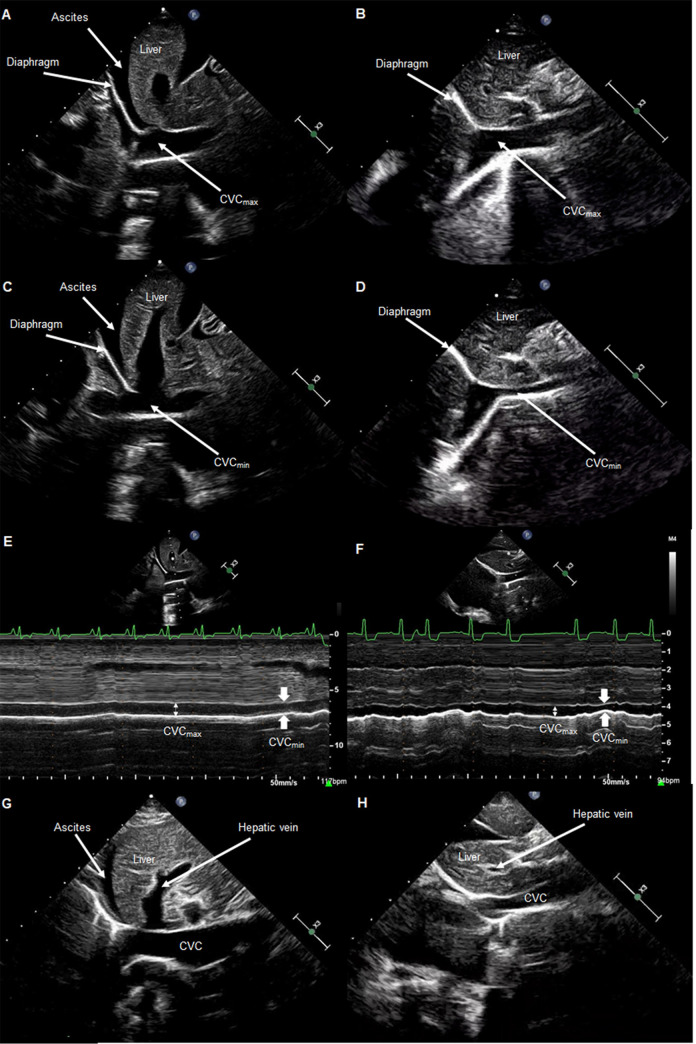
Materials and methods: 113 dogs diagnosed with R-CHF (n = 51), L-CHF (30), or NC effusion (32) were enrolled. Seventeen of the R-CHF dogs had pericardial effusion and tamponade. Focused ultrasound was performed prospectively to obtain 2-dimensional and M-mode subxiphoid measures of CVC maximal and minimal size (CVCmax and CVCmin), CVCmax indexed to aortic dimension (CVC:Ao), and CVC collapsibility index (CVC-CI). Variables were compared between study groups using Kruskal-Wallis and Dunn's-Bonferroni testing, and receiver operating characteristics curves were used to assess sensitivity and specificity.
Results: All sonographic CVC indices were significantly different between R-CHF and NC dogs (P < 0.001). Variables demonstrating the highest diagnostic accuracy for discriminating R-CHF versus NC were CVC-CI <33% in 2D (91% sensitive and 96% specific) and presence of hepatic venous distension (84% sensitive and 90% specific). L-CHF dogs had higher CVC:Ao and lower CVC-CI compared to NC dogs (P = 0.016 and P = 0.043 in 2D, respectively) but increased CVC-CI compared to the R-CHF group (P < 0.001).
Conclusions: Ultrasonographic indices of CVC size and collapsibility differed between dogs with R-CHF compared to NC causes of cavitary effusions. Dogs with L-CHF have CVC measurements intermediate between R-CHF and NC dogs.
Conflict of interest statement
I have read the journal’s policy and the authors of this manuscript have the following competing interests: Dr. Lisciandro is the owner of FASTVet.com, a private corporation that provides veterinary ultrasound training to practicing veterinarians. Ultrasound companies sponsor Global FAST Courses and include Universal Imaging, EI Medical, and Sound; and EI Medical has licensed Global FAST education materials. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
Similar articles
-
Echocardiographic caudal vena cava measurements in healthy cats and in cats with congestive heart failure and non-cardiac causes of cavitary effusions.J Vet Cardiol. 2023 Aug;48:7-18. doi: 10.1016/j.jvc.2023.05.004. Epub 2023 May 10. J Vet Cardiol. 2023. PMID: 37276765
-
Ultrasonographic evaluation of the caudal vena cava in dogs with right-sided heart disease.J Vet Cardiol. 2021 Apr;34:80-92. doi: 10.1016/j.jvc.2021.01.005. Epub 2021 Jan 24. J Vet Cardiol. 2021. PMID: 33626419
-
Caudal vena cava point-of-care ultrasound in dogs with degenerative mitral valve disease without clinically important right heart disease.J Vet Cardiol. 2022 Jun;41:18-29. doi: 10.1016/j.jvc.2022.01.001. Epub 2022 Jan 16. J Vet Cardiol. 2022. PMID: 35168168
-
Focused Canine Cardiac Ultrasound.Vet Clin North Am Small Anim Pract. 2021 Nov;51(6):1203-1216. doi: 10.1016/j.cvsm.2021.07.005. Epub 2021 Sep 9. Vet Clin North Am Small Anim Pract. 2021. PMID: 34511294 Review.
-
Pericardial and pleural effusions in congestive heart failure-anatomical, pathophysiologic, and clinical considerations.Am J Med Sci. 2009 Sep;338(3):211-6. doi: 10.1097/MAJ.0b013e3181a3936f. Am J Med Sci. 2009. PMID: 19574887 Review.
Cited by
-
Role of the inferior vena cava collapsibility index in predicting propofol-induced hypotension in patients undergoing colonoscopy.BMC Anesthesiol. 2025 Feb 14;25(1):73. doi: 10.1186/s12871-025-02945-y. BMC Anesthesiol. 2025. PMID: 39953383 Free PMC article.
-
Effectiveness of 2-dimensional shear wave elastography for noninvasive and reliable estimation of right atrial pressure in dogs with induced volume overload.J Vet Intern Med. 2023 May-Jun;37(3):866-874. doi: 10.1111/jvim.16705. Epub 2023 Apr 10. J Vet Intern Med. 2023. PMID: 37036333 Free PMC article.
-
Utility of focused cardiac ultrasonography training in veterinary students to differentiate stages of subclinical myxomatous mitral valve disease in dogs.J Vet Intern Med. 2024 May-Jun;38(3):1325-1333. doi: 10.1111/jvim.17056. Epub 2024 Mar 27. J Vet Intern Med. 2024. PMID: 38532734 Free PMC article.
-
Retrospective evaluation of the etiology and clinical characteristics of peripheral edema in dogs.J Vet Intern Med. 2023 Sep-Oct;37(5):1725-1737. doi: 10.1111/jvim.16815. Epub 2023 Jul 15. J Vet Intern Med. 2023. PMID: 37452610 Free PMC article.
-
N-terminal brain natriuretic peptide, cardiac troponin-I, and point-of-care ultrasound in dogs with cardiac and noncardiac causes of nonhemorrhagic ascites.J Vet Intern Med. 2023 May-Jun;37(3):900-909. doi: 10.1111/jvim.16702. Epub 2023 Apr 15. J Vet Intern Med. 2023. PMID: 37060291 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
