

Vascular histopathology and connective tissue ultrastructure in spontaneous coronary artery dissection: pathophysiological and clinical implications
- PMID: 34048532
- PMCID: PMC9215198
- DOI: 10.1093/cvr/cvab183
Vascular histopathology and connective tissue ultrastructure in spontaneous coronary artery dissection: pathophysiological and clinical implications
Erratum in
-
Erratum to: Vascular histopathology and connective tissue ultrastructure in spontaneous coronary artery dissection: pathophysiological and clinical implications.Cardiovasc Res. 2023 May 2;119(3):880. doi: 10.1093/cvr/cvac070. Cardiovasc Res. 2023. PMID: 35553642 Free PMC article. No abstract available.
Abstract
Aims: Spontaneous coronary artery dissection (SCAD) is a cause of acute coronary syndromes and in rare cases sudden cardiac death (SCD). Connective tissue abnormalities, coronary inflammation, increased coronary vasa vasorum (VV) density, and coronary fibromuscular dysplasia have all been implicated in the pathophysiology of SCAD but have not previously been systematically assessed. We designed a study to investigate the coronary histological and dermal collagen ultrastructural findings in SCAD.
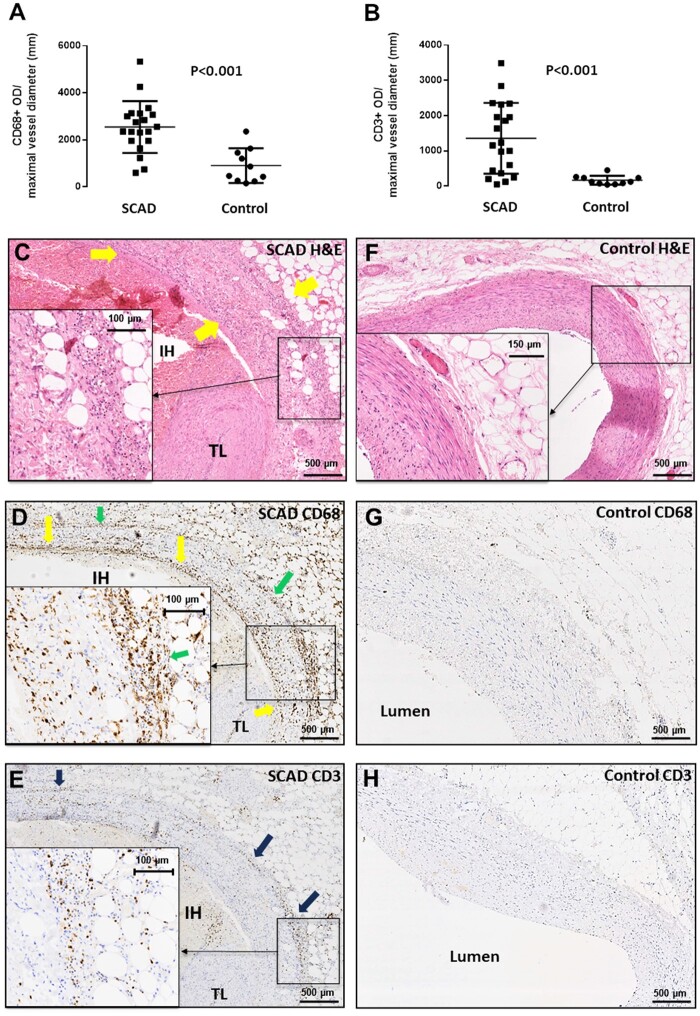
Methods and results: Thirty-six autopsy SCAD cases were compared with 359 SCAD survivors. Coronary and myocardial histology and immunohistochemistry were undertaken. Transmission electron microscopy (TEM) of dermal extracellular matrix (ECM) components of n = 31 SCAD survivors and n = 16 healthy volunteers were compared. Autopsy cases were more likely male (19% vs. 5%; P = 0.0004) with greater proximal left coronary involvement (56% vs. 18%; P < 0.0001) compared to SCAD survivors. N = 24 (66%) of cases showed no myocardial infarction on macro- or microscopic examination consistent with arrhythmogenic death. There was significantly (P < 0.001) higher inflammation in cases with delayed-onset death vs. sudden death and significantly more inflammation surrounding the dissected vs. non-dissected vessel segments. N = 17 (47%) cases showed limited intimal fibro-elastic thickening but no features of fibromuscular dysplasia and no endothelial or internal elastic lamina abnormalities. There were no differences in VV density between SCAD and control cases. TEM revealed no general ultrastructural differences in ECM components or markers of fibroblast metabolic activity.
Conclusions: Assessment of SCD requires careful exclusion of SCAD, particularly in cases without myocardial necrosis. Peri-coronary inflammation in SCAD is distinct from vasculitides and likely a reaction to, rather than a cause for SCAD. Coronary fibromuscular dysplasia or increased VV density does not appear pathophysiologically important. Dermal connective tissue changes are not common in SCAD survivors.
Keywords: Autopsy; Collagen; Electron microscopy; Haematoma; Inflammation; Spontaneous coronary artery dissection; Sudden cardiac death; Vascular.
© The Author(s) 2021. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures







Comment in
-
Is there more than meets the eye? Spontaneous coronary artery dissection and sudden cardiac death.Cardiovasc Res. 2022 Jun 22;118(7):1615-1617. doi: 10.1093/cvr/cvac043. Cardiovasc Res. 2022. PMID: 35425981 No abstract available.
References
-
- Hayes SN, Kim ESH, Saw J, Adlam D, Arslanian-Engoren C, Economy KE, Ganesh SK, Gulati R, Lindsay ME, Mieres JH, Naderi S, Shah S, Thaler DE, Tweet MS, Wood MJ; American Heart Association Council on Peripheral Vascular Disease; Council on Clinical Cardiology; Council on Cardiovascular and Stroke Nursing; Council on Genomic and Precision Medicine; and Stroke Council . Spontaneous coronary artery dissection: current state of the science: a scientific statement from the American Heart Association. Circulation 2018;137:e523–e557. - PMC - PubMed
-
- Desai S, Sheppard MN.. Sudden cardiac death: look closely at the coronaries for spontaneous dissection which can be missed. A study of 9 cases. Am J Forensic Med Pathol 2012;33:26–29. - PubMed
-
- Vrints CJ. Spontaneous coronary artery dissection. Heart 2010;96:801–808. - PubMed
-
- Kwon TG, Gulati R, Matsuzawa Y, Aoki T, Guddeti RR, Herrmann J, Lennon RJ, Ritman EL, Lerman LO, Lerman A.. Proliferation of coronary adventitial vasa vasorum in patients with spontaneous coronary artery dissection. JACC Cardiovasc Imaging 2016;9:891–892. - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
