

Hypothesis for renin-angiotensin inhibitor mitigation of COVID-19
- PMID: 34048987
- PMCID: PMC8114589
- DOI: 10.1016/j.mehy.2021.110609
Hypothesis for renin-angiotensin inhibitor mitigation of COVID-19
Abstract
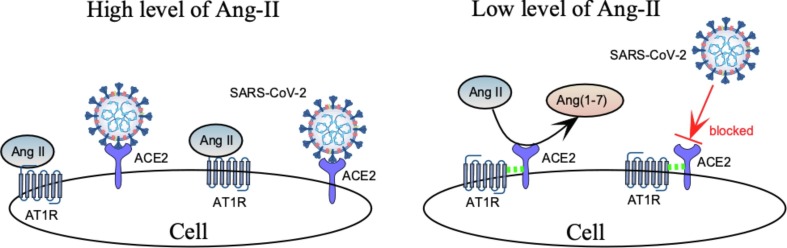
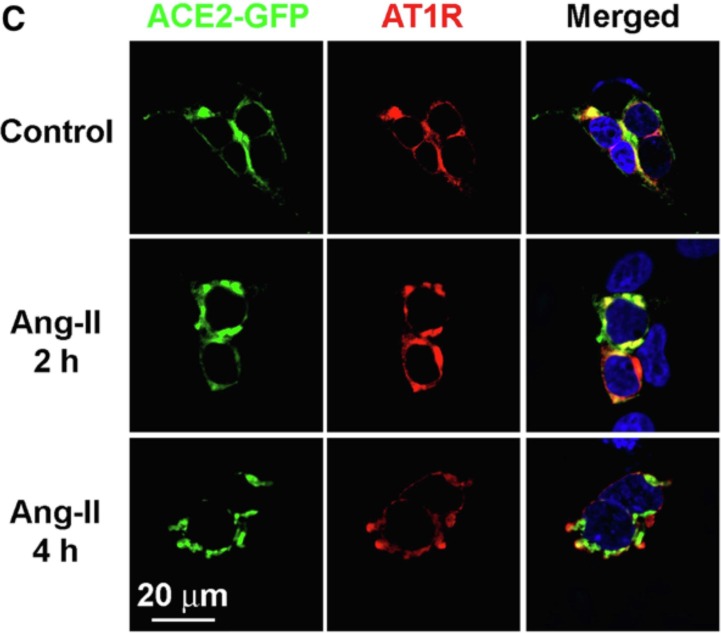
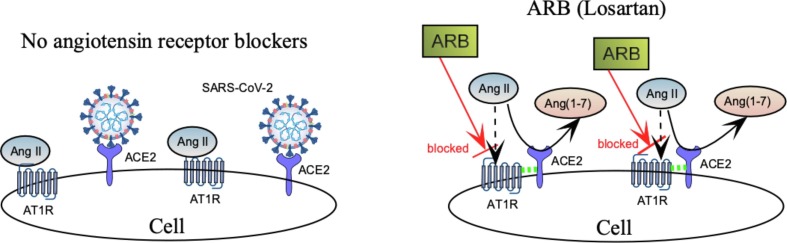
Preexisting hypertension is a known risk factor for severe COVID-19. Abnormal activation of RAS upregulates angiotensin II (Ang-II) and contributes to severe manifestations of COVID-19. Although RAS inhibitors (RASi) are a mainstay of antihypertensive therapy, they have been associated (in some animal studies) with an increase in angiotensin converting enzyme 2 (ACE2) receptors that facilitate cellular entry of the SARS-CoV-2 virus. Nonetheless, current medical practice does not recommend curtailing RASi to protect hypertensive patients from COVID. On the contrary, there is clinical evidence to support a beneficial effect of RASi for hypertensive patients in the midst of a COVID-19 pandemic, although the precise mechanism for this is unclear. In this paper, we hypothesize that RASi reduces the severity of COVID-19 by promoting ACE2-AT1R complex formation at the cell surface, where AT1R mediates the major vasopressor effects of Ang-II. Furthermore, we propose that the interaction between ACE2 and AT1R impedes binding of SARS-CoV-2 to ACE2, thereby allowing ACE2 to convert Ang-II to the more beneficial Ang(1-7), that has vasodilator and anti-inflammatory activity. Evidence for ACE2-AT1R complex formation during reduced Ang-II comes from receptor colocalization studies in isolated HEK293 cells, but this has not been confirmed in cells having endogenous expression of ACE2 and AT1R. Since the SARS-CoV-2 virus attacks the kidney, as well as the heart and lung, our hypothesis for the effect of RASi on COVID-19 could be tested in vitro using human proximal tubule cells (HK-2), having ACE2 and AT1 receptors. Specifically, colocalization of fluorescent labelled: SARS-CoV-2 spike protein, ACE2, and AT1R in HK-2 cells can be used to clarify the mechanism of RASi action in renal and lung epithelia, which could lead to protocols for reducing the severity of COVID-19 in both hypertensive and normotensive patients.
Keywords: ACE2; Angiotensin; Hypertension; Kidney; RAS; Renin; SARS-CoV-2.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Sun M., Yang J., Sun Y., Su G. Inhibitors of RAS Might Be a Good Choice for the Therapy of COVID-19 Pneumonia. Chin J Tuberc Respir Dis. 2020;43 Epub ahead of print. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
