

Assessment of cognitive and psychomotor impairment, subjective effects, and blood THC concentrations following acute administration of oral and vaporized cannabis
- PMID: 34049452
- PMCID: PMC9361180
- DOI: 10.1177/02698811211021583
Assessment of cognitive and psychomotor impairment, subjective effects, and blood THC concentrations following acute administration of oral and vaporized cannabis
Abstract
Background: Cannabis legalization is expanding, but there are no established methods for detecting cannabis impairment.
Aim: Characterize the acute impairing effects of oral and vaporized cannabis using various performance tests.
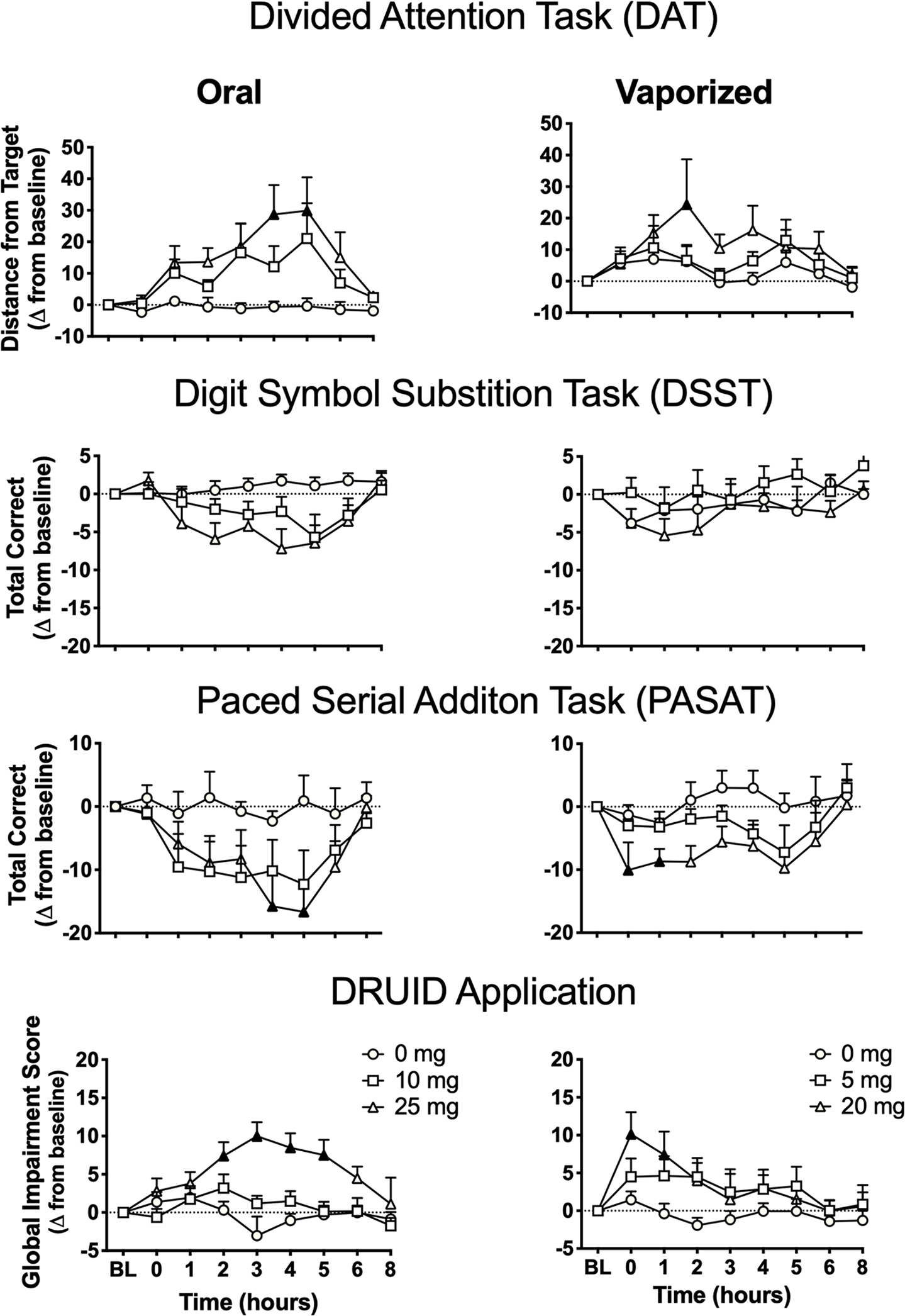
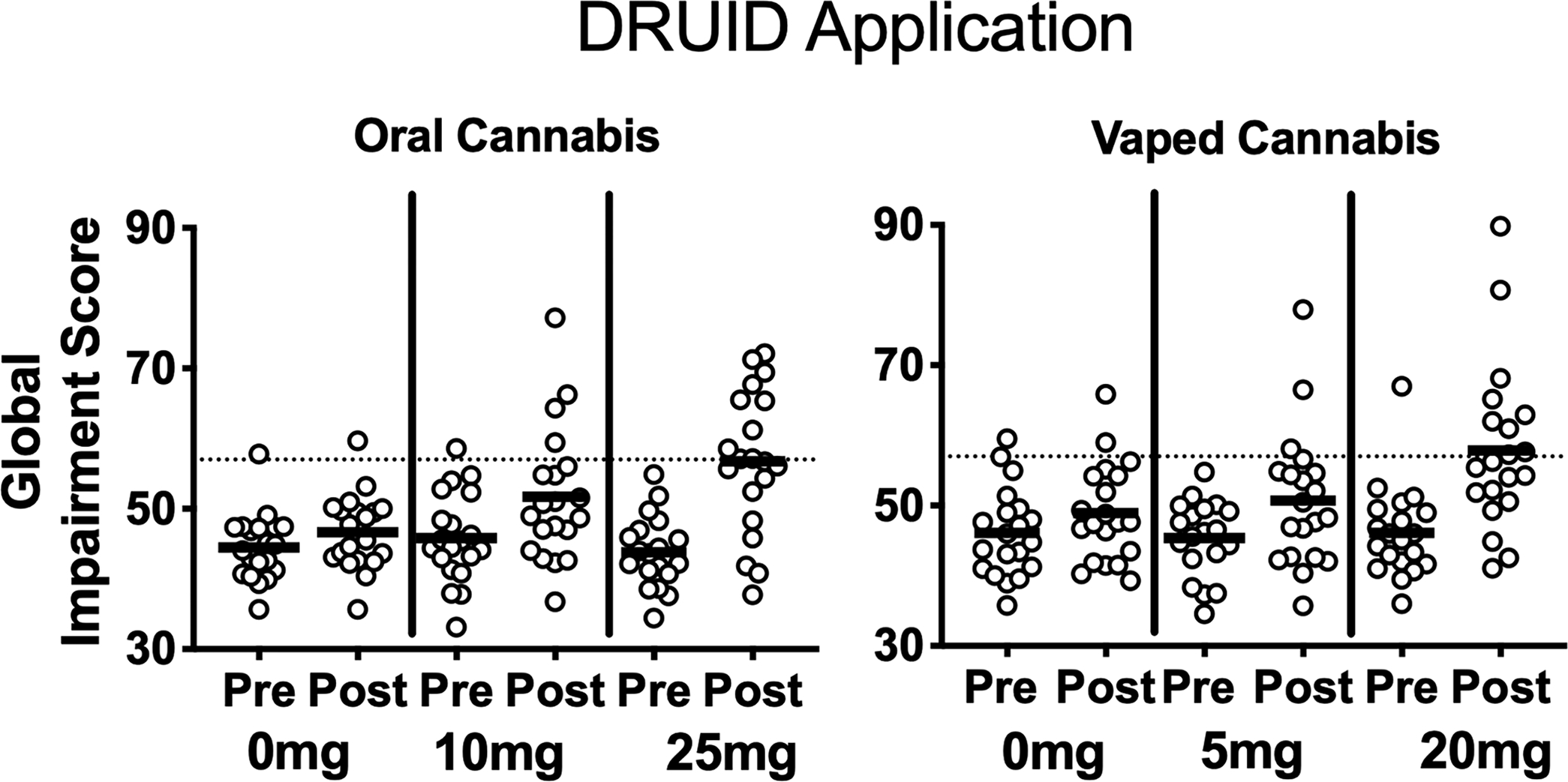
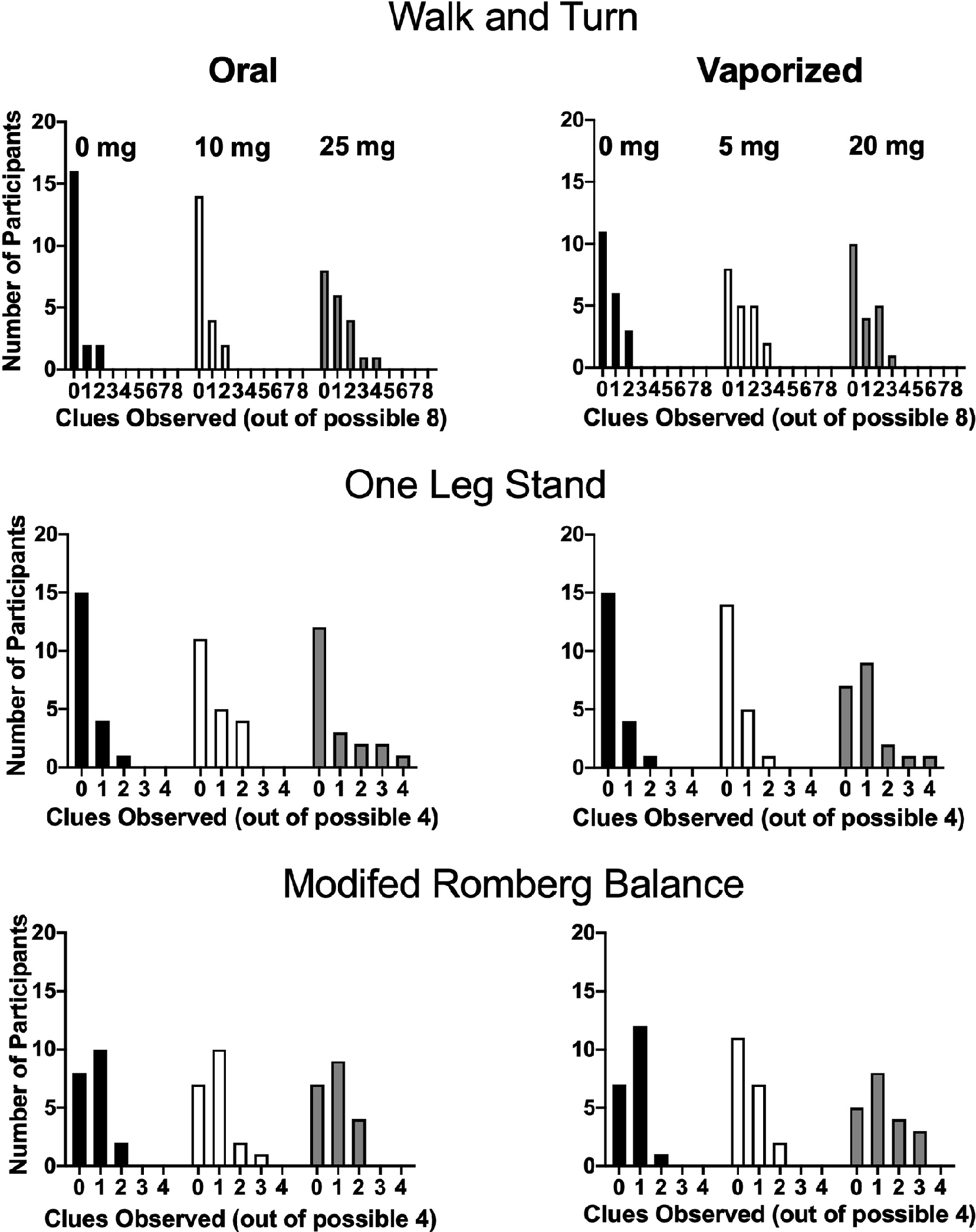
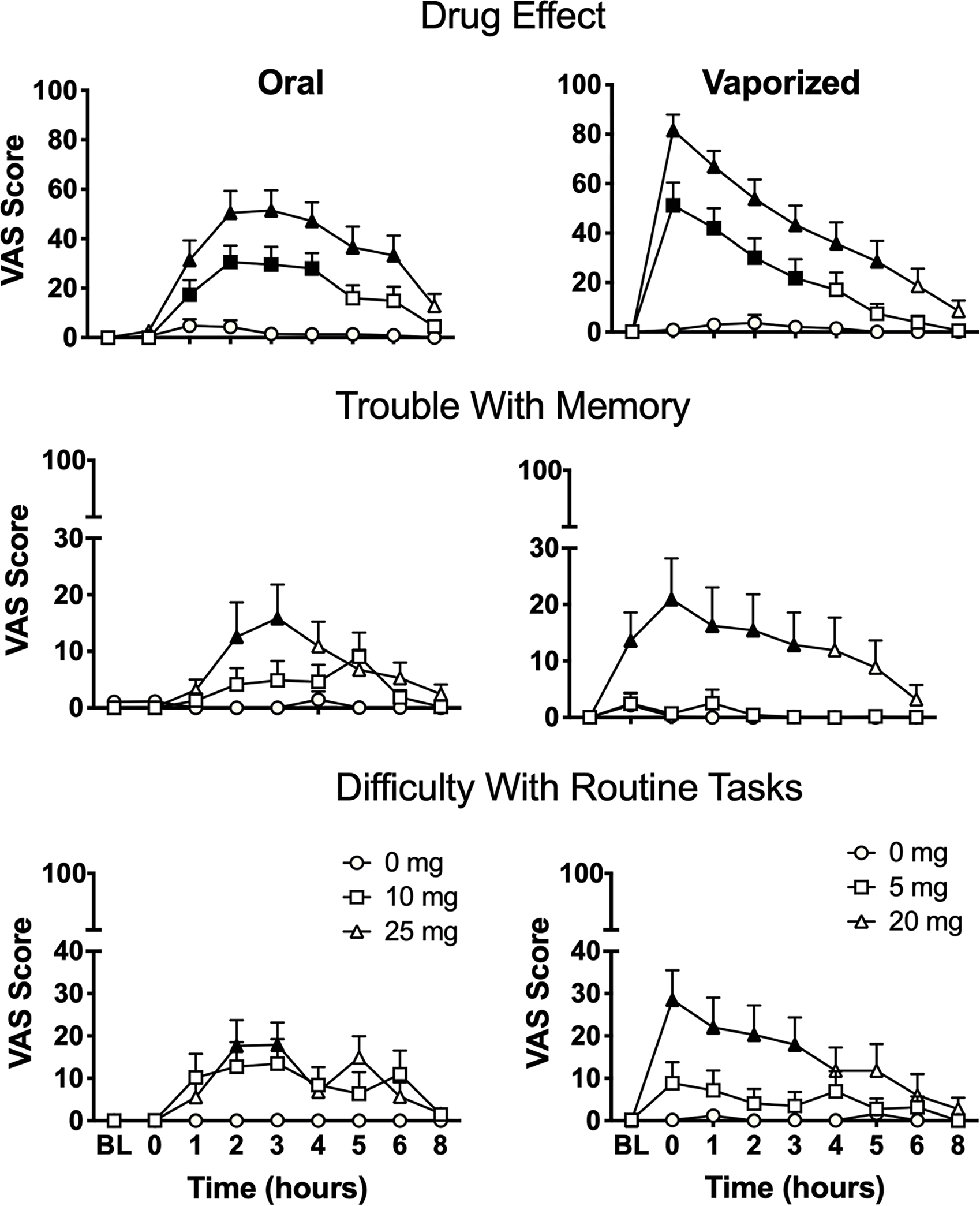
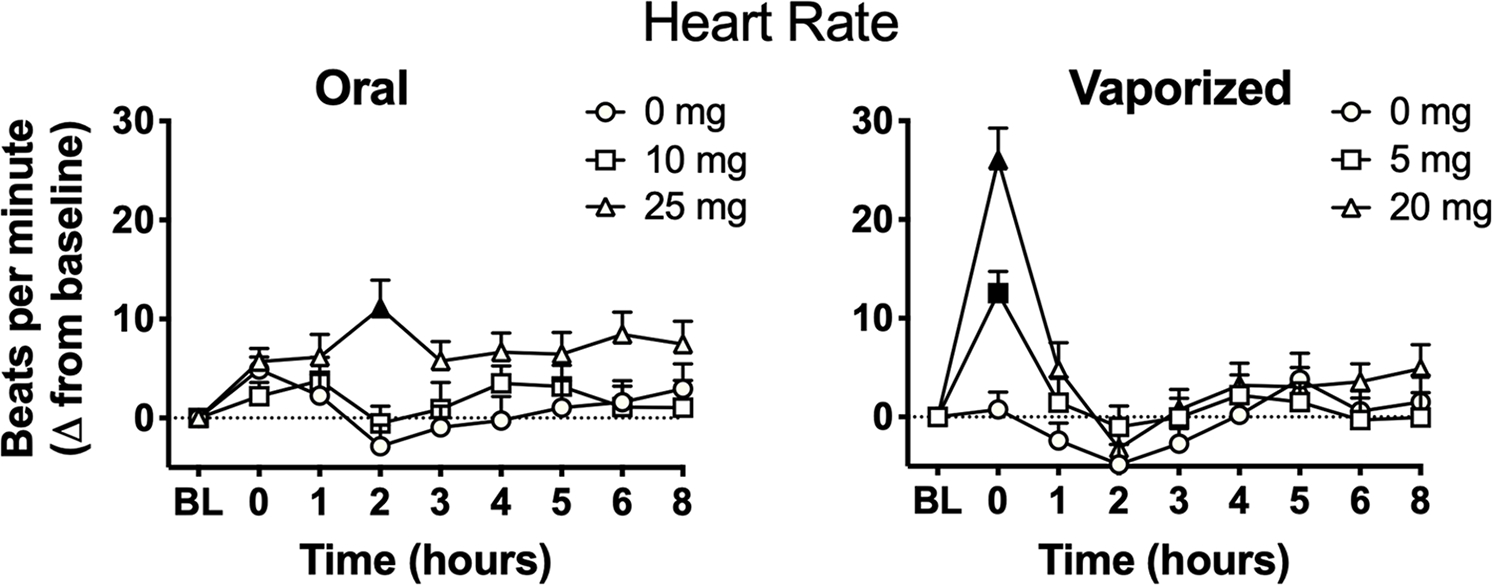
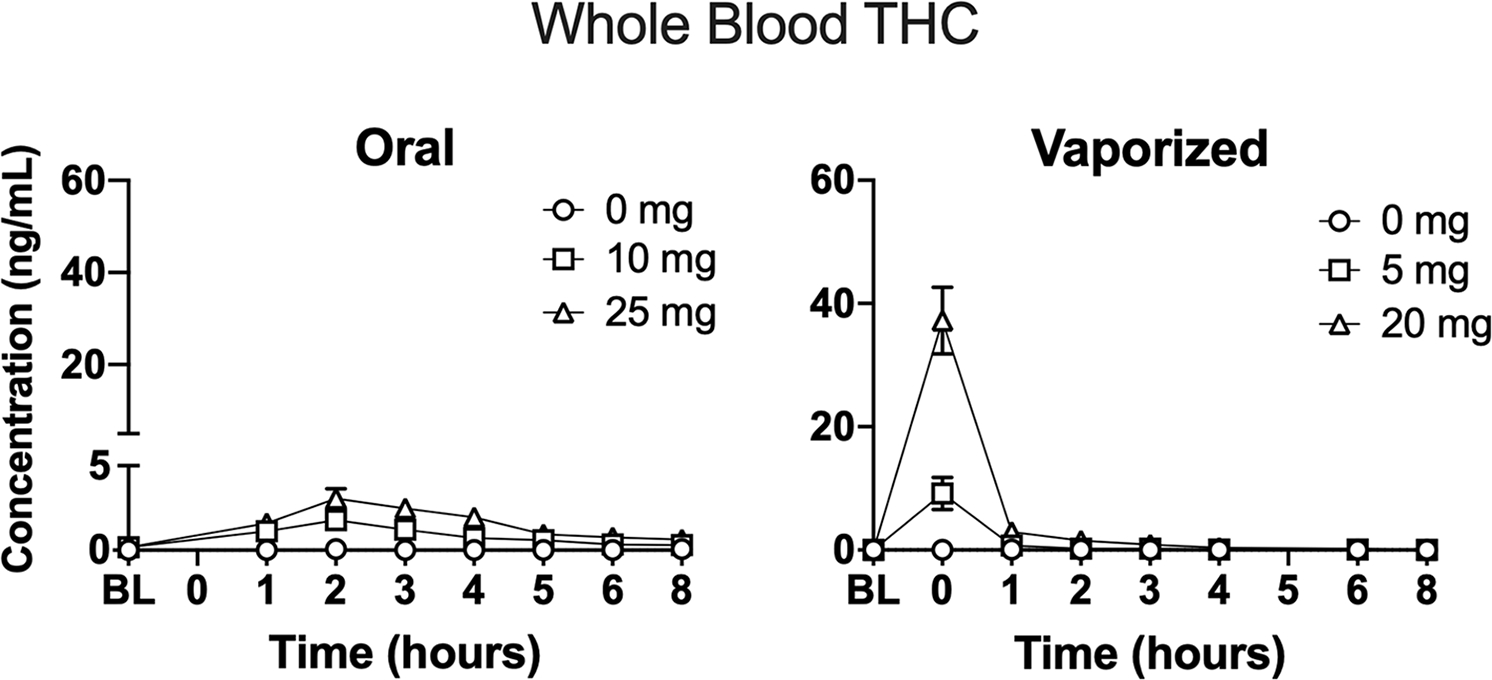
Methods: Participants (N = 20, 10 men/10 women) who were infrequent cannabis users ingested cannabis brownies (0, 10, and 25 mg Δ-9-tetrahydrocannabinol, THC) and inhaled vaporized cannabis (0, 5, and 20 mg THC) in six double-blind outpatient sessions. Cognitive/psychomotor impairment was assessed with a battery of computerized tasks sensitive to cannabis effects, a novel test (the DRiving Under the Influence of Drugs, DRUID®), and field sobriety tests. Blood THC concentrations and subjective drug effects were evaluated.
Results: Low oral/vaporized doses did not impair cognitive/psychomotor performance relative to placebo but produced positive subjective effects. High oral/vaporized doses impaired cognitive/psychomotor performance and increased positive and negative subjective effects. The DRUID® was the most sensitive test to cannabis impairment, as it detected significant differences between placebo and active doses within both routes of administration. Women displayed more impairment on the DRUID® than men at the high vaporized dose only. Field sobriety tests showed little sensitivity to cannabis-induced impairment. Blood THC concentrations were far lower after cannabis ingestion versus inhalation. After inhalation, blood THC concentrations typically returned to baseline well before pharmacodynamic effects subsided.
Conclusions: Standard approaches for identifying impairment due to cannabis exposure (i.e. blood THC and field sobriety tests) have severe limitations. There is a need to identify novel biomarkers of cannabis exposure and/or behavioral tests like the DRUID® that can reliably and accurately detect cannabis impairment at the roadside and in the workplace.
Keywords: Cannabis; cannabis edibles; cannabis vaporizers; impairment.
Conflict of interest statement
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Spindle has served as a consultant for Canopy Health Innovations Inc. Dr. Vandrey has served as a consultant or received honoraria from Canopy Health Innovations Inc., FSD Pharma, and Present Life Corporation. Michael Milburn is the creator of the DRUID® application and is the Chief Scientific Officer (CSO) and a stockholder of Impairment Science, Inc. The remaining authors have no conflicts of interest to declare.
Figures
Similar articles
-
Pharmacodynamic effects of vaporized and oral cannabidiol (CBD) and vaporized CBD-dominant cannabis in infrequent cannabis users.Drug Alcohol Depend. 2020 Jun 1;211:107937. doi: 10.1016/j.drugalcdep.2020.107937. Epub 2020 Apr 1. Drug Alcohol Depend. 2020. PMID: 32247649 Free PMC article.
-
Acute Effects of Smoked and Vaporized Cannabis in Healthy Adults Who Infrequently Use Cannabis: A Crossover Trial.JAMA Netw Open. 2018 Nov 2;1(7):e184841. doi: 10.1001/jamanetworkopen.2018.4841. JAMA Netw Open. 2018. PMID: 30646391 Free PMC article. Clinical Trial.
-
A within-subject cross-over trial comparing the acute effects of vaporized delta-8-tetrahydrocannabinol and delta-9-tetrahydrocannabinol in healthy adults.Drug Alcohol Depend. 2025 Jul 1;272:112684. doi: 10.1016/j.drugalcdep.2025.112684. Epub 2025 Apr 21. Drug Alcohol Depend. 2025. PMID: 40334328 Clinical Trial.
-
Are blood and oral fluid Δ9-tetrahydrocannabinol (THC) and metabolite concentrations related to impairment? A meta-regression analysis.Neurosci Biobehav Rev. 2022 Mar;134:104433. doi: 10.1016/j.neubiorev.2021.11.004. Epub 2021 Nov 9. Neurosci Biobehav Rev. 2022. PMID: 34767878 Review.
-
Cannabis use: a perspective in relation to the proposed UK drug-driving legislation.Drug Test Anal. 2014 Jan-Feb;6(1-2):143-54. doi: 10.1002/dta.1588. Epub 2013 Dec 11. Drug Test Anal. 2014. PMID: 24327278 Review.
Cited by
-
Urinary Excretion Profile of Cannabinoid Analytes Following Acute Administration of Oral and Vaporized Cannabis in Infrequent Cannabis Users.J Anal Toxicol. 2022 Oct 14;46(8):882-890. doi: 10.1093/jat/bkac042. J Anal Toxicol. 2022. PMID: 35770374 Free PMC article. Clinical Trial.
-
Identification of ∆9-tetrahydrocannabinol (THC) impairment using functional brain imaging.Neuropsychopharmacology. 2022 Mar;47(4):944-952. doi: 10.1038/s41386-021-01259-0. Epub 2022 Jan 8. Neuropsychopharmacology. 2022. PMID: 34999737 Free PMC article. Clinical Trial.
-
Medical Cannabis Use Patterns for Sleep Disorders in Australia: Results of the Cross-Sectional CAMS-20 Survey.Nat Sci Sleep. 2023 Apr 17;15:245-255. doi: 10.2147/NSS.S390583. eCollection 2023. Nat Sci Sleep. 2023. PMID: 37090897 Free PMC article.
-
Preliminary study of the interactive effects of THC and ethanol on self-reported ability and simulated driving, subjective effects, and cardiovascular responses.Psychopharmacology (Berl). 2023 Jun;240(6):1235-1246. doi: 10.1007/s00213-023-06356-0. Epub 2023 Apr 12. Psychopharmacology (Berl). 2023. PMID: 37045988 Clinical Trial.
-
Effects of recent cannabis consumption on eye-tracking and pupillometry.Front Neurosci. 2024 Apr 9;18:1358491. doi: 10.3389/fnins.2024.1358491. eCollection 2024. Front Neurosci. 2024. PMID: 38655106 Free PMC article.
References
-
- Abrams DI, Vizoso HP, Shade SB, et al. (2007) Vaporization as a smokeless cannabis delivery system: A pilot study. Clin Pharmacol Ther 82: 572–578. - PubMed
-
- Bosker WM, Kuypers KP, Theunissen EL, et al. (2012) Medicinal Delta(9)-tetrahydrocannabinol (dronabinol) impairs on-the-road driving performance of occasional and heavy cannabis users but is not detected in Standard Field Sobriety Tests. Addiction 107: 1837–1844. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
