

Standard of care for lipedema in the United States
- PMID: 34049453
- PMCID: PMC8652358
- DOI: 10.1177/02683555211015887
Standard of care for lipedema in the United States
Abstract
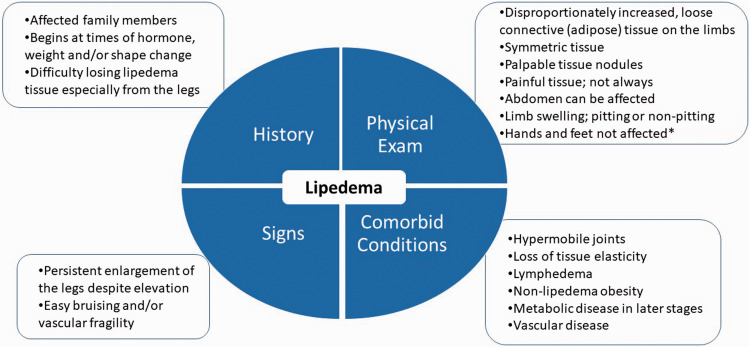
Background: Lipedema is a loose connective tissue disease predominantly in women identified by increased nodular and fibrotic adipose tissue on the buttocks, hips and limbs that develops at times of hormone, weight and shape change including puberty, pregnancy, and menopause. Lipedema tissue may be very painful and can severely impair mobility. Non-lipedema obesity, lymphedema, venous disease, and hypermobile joints are comorbidities. Lipedema tissue is difficult to reduce by diet, exercise, or bariatric surgery.
Methods: This paper is a consensus guideline on lipedema written by a US committee following the Delphi Method. Consensus statements are rated for strength using the GRADE system.
Results: Eighty-five consensus statements outline lipedema pathophysiology, and medical, surgical, vascular, and other therapeutic recommendations. Future research topics are suggested.
Conclusion: These guidelines improve the understanding of the loose connective tissue disease, lipedema, to advance our understanding towards early diagnosis, treatments, and ultimately a cure for affected individuals.
Keywords: Lipedema; chronic venous disease; hypermobility; lymphedema; standard of care.
Conflict of interest statement
Figures
References
-
- Felmerer G, Stylianaki A, Hägerling R, et al. Adipose tissue hypertrophy, an aberrant biochemical profile and distinct gene expression in lipedema. J Surg Res 2020; 253: 294–303. - PubMed
-
- Herbst K, Mirkovskaya L, Bharhagava A, et al. Lipedema fat and signs and symptoms of illness, increase with advancing stage. Arch Med 2015; 7: 1–8.
-
- Allen EV, Hines EAJ. Lipedema of the legs: a syndrome characterised by fat legs and orthostatic edema. Proc Staff Meet Mayo Clin 1940; 15: 184–187.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
