

Accuracy of pancreatic stone protein for the diagnosis of infection in hospitalized adults: a systematic review and individual patient level meta-analysis
- PMID: 34049579
- PMCID: PMC8164316
- DOI: 10.1186/s13054-021-03609-2
Accuracy of pancreatic stone protein for the diagnosis of infection in hospitalized adults: a systematic review and individual patient level meta-analysis
Abstract
Background: Accurate biomarkers to diagnose infection are lacking. Studies reported good performance of pancreatic stone protein (PSP) to detect infection. The objective of the study was to determine the performance of PSP in diagnosing infection across hospitalized patients and calculate a threshold value for that purpose.
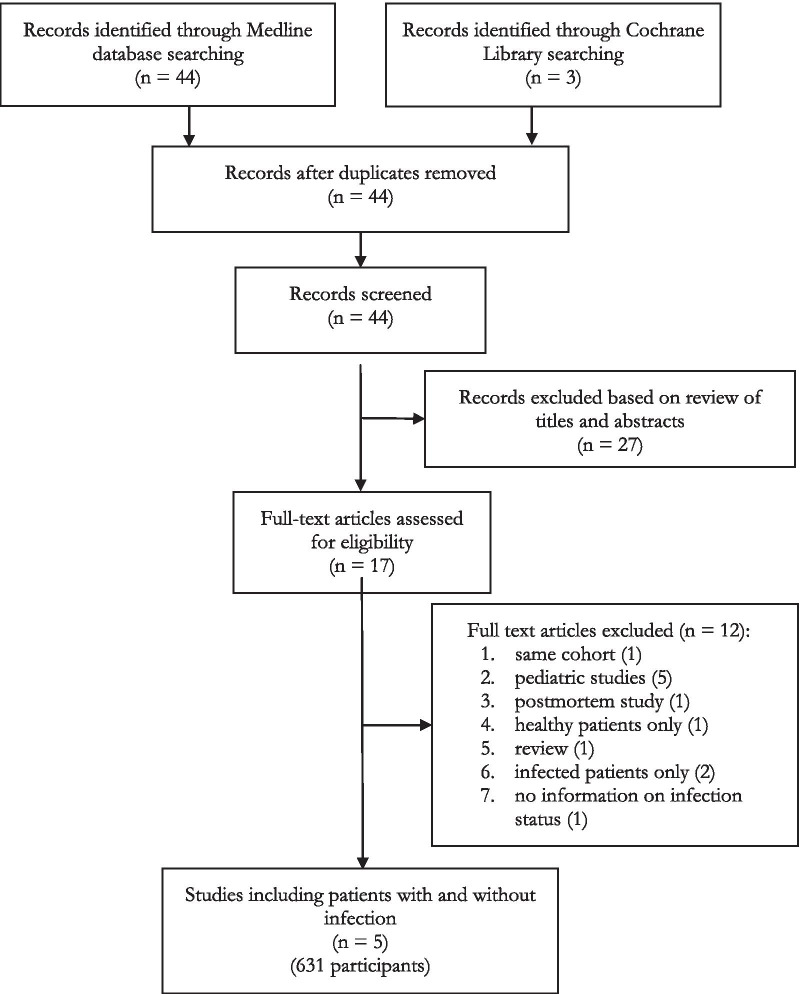
Methods: A systematic search across Cochrane Central Register of Controlled Trials and MEDLINE databases (1966-March 2019) for studies on PSP published in English using 'pancreatic stone protein', 'PSP', 'regenerative protein', 'lithostatin' combined with 'infection' and 'sepsis' found 44 records. The search was restricted to the five trials that evaluated PSP for the initial detection of infection in hospitalized adults. Individual patient data were obtained from the investigators of all eligible trials. Data quality and validity was assessed according to PRISMA guidelines. We choose a fixed-effect model to calculate the PSP cut-off value that best discriminates infected from non-infected patients.
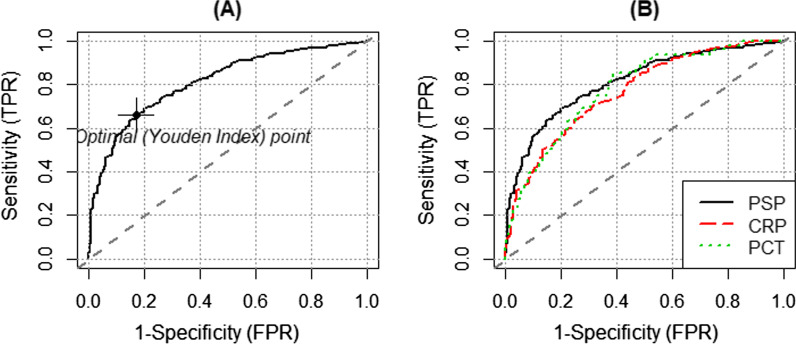
Results: Infection was confirmed in 371 of 631 patients. The median (IQR) PSP value of infected versus uninfected patients was 81.5 (30.0-237.5) versus 19.2 (12.6-33.57) ng/ml, compared to 150 (82.70-229.55) versus 58.25 (15.85-120) mg/l for C-reactive protein (CRP) and 0.9 (0.29-4.4) versus 0.15 (0.08-0.5) ng/ml for procalcitonin (PCT). Using a PSP cut-off of 44.18 ng/ml, the ROC AUC to detect infection was 0.81 (0.78-0.85) with a sensitivity of 0.66 (0.61-0.71), specificity of 0.83 (0.78-0.88), PPV of 0.85 (0.81-0.89) and NPV of 0.63 (0.58-0.68). When a model combining PSP and CRP was used, the ROC AUC improved to 0.90 (0.87-0.92) with higher sensitivity 0.81 (0.77-0.85) and specificity 0.84 (0.79-0.90) for discriminating infection from non-infection. Adding PCT did not improve the performance further.
Conclusions: PSP is a promising biomarker to diagnose infections in hospitalized patients. Using a cut-off value of 44.18 ng/ml, PSP performs better than CRP or PCT across the considered studies. The combination of PSP with CRP further enhances its accuracy.
Keywords: Biomarker; Infection; PSP; Pancreatic stone protein.
Conflict of interest statement
All authors have completed the ICMJE uniform disclosure form at
Figures
Similar articles
-
Discriminative performance of pancreatic stone protein in predicting ICU mortality and infection severity in adult patients with infection: a systematic review and individual patient level meta-analysis.Infection. 2023 Dec;51(6):1797-1807. doi: 10.1007/s15010-023-02093-w. Epub 2023 Sep 14. Infection. 2023. PMID: 37707744 Free PMC article.
-
Serial measurement of pancreatic stone protein for the early detection of sepsis in intensive care unit patients: a prospective multicentric study.Crit Care. 2021 Apr 20;25(1):151. doi: 10.1186/s13054-021-03576-8. Crit Care. 2021. PMID: 33879189 Free PMC article.
-
Prognostic Value of High-Sensitivity C-Reactive Protein, Procalcitonin and Pancreatic Stone Protein in Pediatric Sepsis.Med Sci Monit. 2017 Mar 30;23:1533-1539. doi: 10.12659/msm.900856. Med Sci Monit. 2017. PMID: 28358790 Free PMC article.
-
Accuracy of Pancreatic Stone Protein for diagnosis of sepsis in children admitted to pediatric intensive care or high-dependency care: a pilot study.Ital J Pediatr. 2023 Oct 7;49(1):134. doi: 10.1186/s13052-023-01540-6. Ital J Pediatr. 2023. PMID: 37805604 Free PMC article.
-
Measurement of pancreatic stone protein in the identification and management of sepsis.Biomark Med. 2019 Feb;13(2):135-145. doi: 10.2217/bmm-2018-0194. Epub 2019 Jan 23. Biomark Med. 2019. PMID: 30672312 Review.
Cited by
-
Sepsis Biomarkers: Advancements and Clinical Applications-A Narrative Review.Int J Mol Sci. 2024 Aug 19;25(16):9010. doi: 10.3390/ijms25169010. Int J Mol Sci. 2024. PMID: 39201697 Free PMC article. Review.
-
Neutrophil Extracellular Traps in the Prognosis of Sepsis: A Current Update.Medicina (Kaunas). 2025 Jun 25;61(7):1145. doi: 10.3390/medicina61071145. Medicina (Kaunas). 2025. PMID: 40731775 Free PMC article. Review.
-
Pancreatic stone protein as a novel biomarker of microvascular complications in type II diabetes mellitus: A systematic review and meta-analysis.Tzu Chi Med J. 2025 Mar 5;37(3):328-338. doi: 10.4103/tcmj.tcmj_211_24. eCollection 2025 Jul-Sep. Tzu Chi Med J. 2025. PMID: 40741607 Free PMC article.
-
The critical role of pancreatic stone protein/regenerating protein in sepsis-related multiorgan failure.Front Med (Lausanne). 2023 May 5;10:1172529. doi: 10.3389/fmed.2023.1172529. eCollection 2023. Front Med (Lausanne). 2023. PMID: 37215716 Free PMC article.
-
Diagnostic and Prognostic Ability of Pancreatic Stone Protein: A Scoping Review.Int J Mol Sci. 2024 May 31;25(11):6046. doi: 10.3390/ijms25116046. Int J Mol Sci. 2024. PMID: 38892234 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
