

Evidence-based prediction and prevention of cardiovascular morbidity in adults treated for cancer
- PMID: 34049593
- PMCID: PMC8161987
- DOI: 10.1186/s40959-021-00105-y
Evidence-based prediction and prevention of cardiovascular morbidity in adults treated for cancer
Abstract
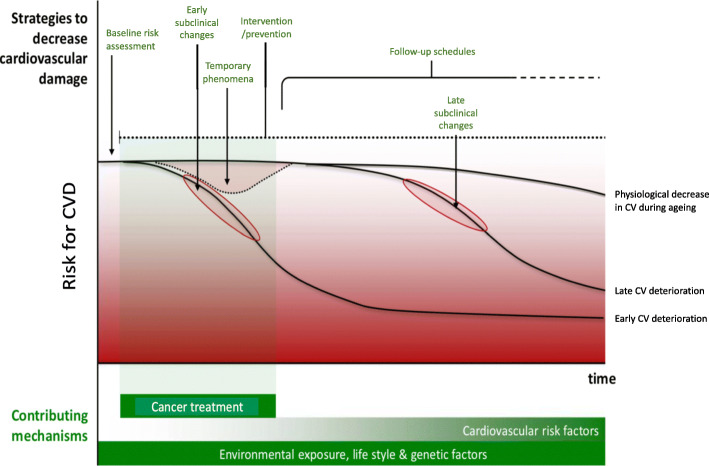
Background: Cancer treatment-related morbidity relevantly compromises health status in cancer survivors, and efforts to optimise health-related outcomes in this population are vital to maximising healthy survivorship. A pre-treatment assessment - and possibly preventive management strategies - of cancer patients at increased risk for cardiovascular disease (CVD) seems a rational approach in this regard. Definitive evidence for such strategies is largely lacking, thereby impeding the formulation of firm recommendations.
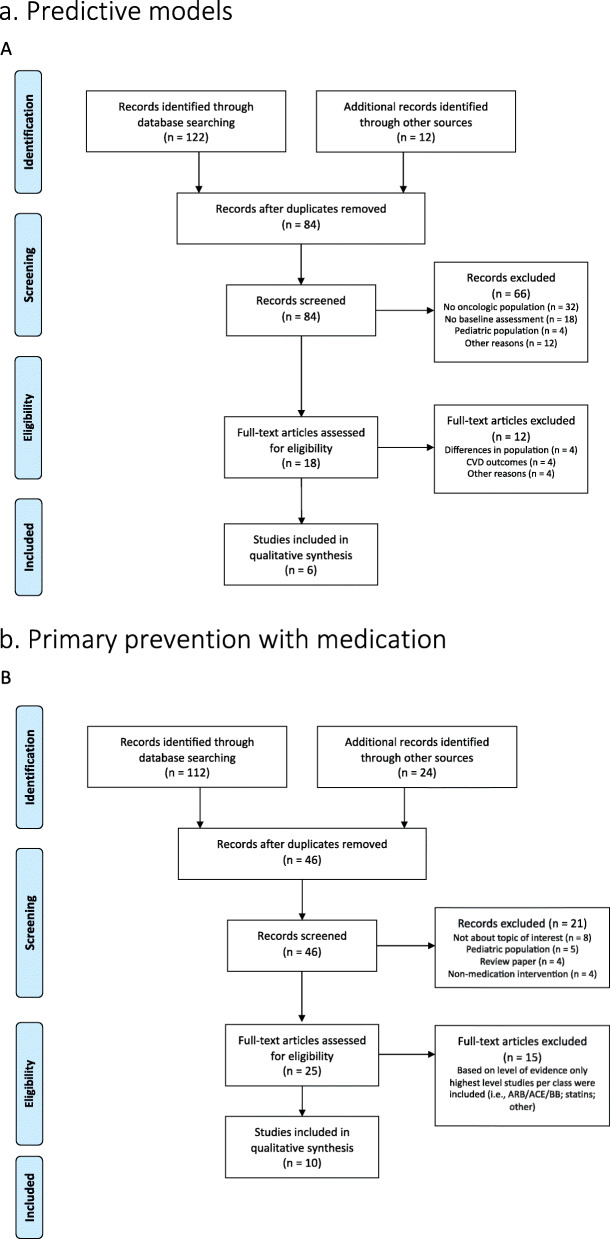
Results: The current scoping review aims to summarise and grade the evidence regarding strategies for prediction and prevention of CVD in adults in relation to oncological treatments. We conducted a scoping literature search for different strategies for primary prevention, such as medical and lifestyle interventions, as well as the use of predictive risk scores. We identified studies with moderate to good strength and up to now limited evidence to recommend primary preventive strategies in unselected patients treated with potentially cardiotoxic oncologic therapies.
Conclusion: Efforts to minimize the CVD burden in cancer survivors are needed to accomplish healthy survivorship. This can be done by means of robust models predictive for CVD events or application of interventions during or after oncological treatments. Up to now there is insufficient evidence to implement preventive strategies in an unselected group of patients treated with potential cardiotoxic oncological treatments. We conclude that randomised controlled trials are needed that evaluate medical and lifestyle interventions in groups at increased risk for complications, in order to be able to influence chronic illness risks, such as cardiovascular complications, for cancer survivors.
Keywords: Cancer survivor; Cardiotoxicity; Evidence-based; Exercise; Lifestyle; Prevention.
Conflict of interest statement
The authors declare that they have no competing interests
Figures
References
-
- Globocan 2018; https://www.uicc.org/news/new-global-cancer-data-globocan-2018. Date Accessed 2019-09-12.
-
- Fitzmaurice, et al. Global burden of disease cancer collaboration. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 29 cancer groups, 1990 to 2016. JAMA Oncol. 2018;4(11):1553. doi: 10.1001/jamaoncol.2018.2706. - DOI - PMC - PubMed
-
- Curigliano G, Burstein HJ, Winer EP, Gnant M, Dubsky P, Loibl S, Colleoni M, Regan MM, Piccart-Gebhart M, Senn HJ, Thürlimann B, St. Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2017. André F, Baselga J, Bergh J, Bonnefoi H, Brucker SY, Cardoso F, Carey L, Ciruelos E, Cuzick J, Denkert C, di Leo A, Ejlertsen B, Francis P, Galimberti V, Garber J, Gulluoglu B, Goodwin P, Harbeck N, Hayes DF, Huang CS, Huober J, Hussein K, Jassem J, Jiang Z, Karlsson P, Morrow M, Orecchia R, Osborne KC, Pagani O, Partridge AH, Pritchard K, Ro J, Rutgers EJT, Sedlmayer F, Semiglazov V, Shao Z, Smith I, Toi M, Tutt A, Viale G, Watanabe T, Whelan TJ, Xu B. De-escalating and escalating treatments for early-stage breast Cancer: the St. Gallen international expert consensus conference on the primary therapy of early breast Cancer 2017. Ann Oncol. 2017;28(8):1700–1712. doi: 10.1093/annonc/mdx308. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources