

Variation in arterial input function in a large multicenter computed tomography perfusion study
- PMID: 34050385
- PMCID: PMC8523411
- DOI: 10.1007/s00330-021-08067-6
Variation in arterial input function in a large multicenter computed tomography perfusion study
Abstract
Objectives: To report the variation in computed tomography perfusion (CTP) arterial input function (AIF) in a multicenter stroke study and to assess the impact this has on CTP results.
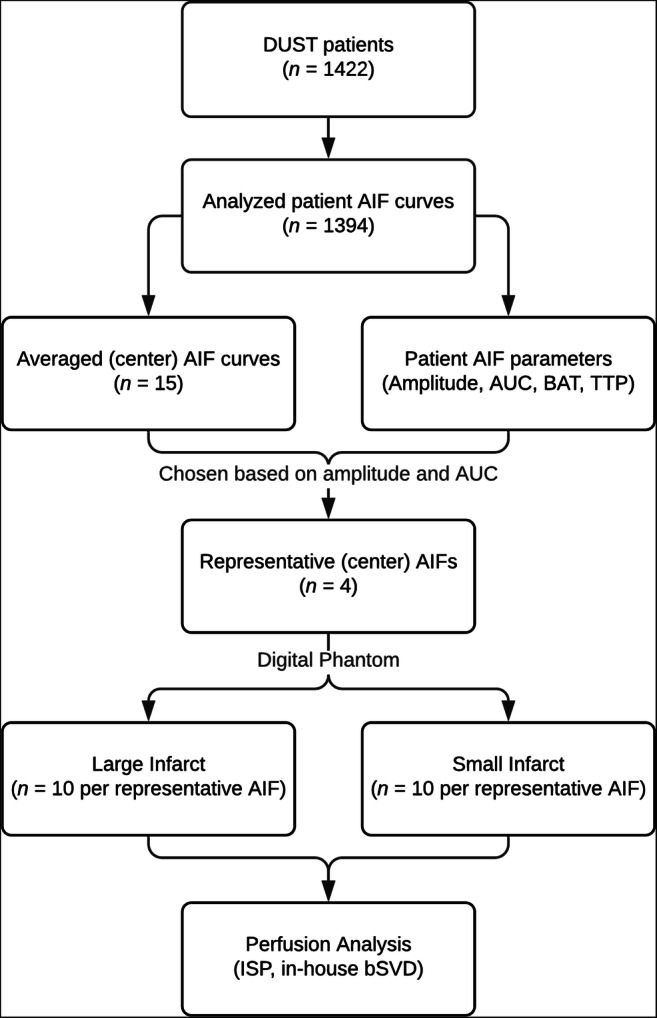
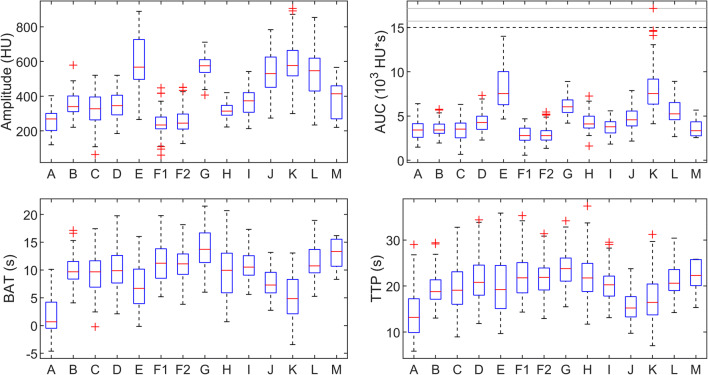
Methods: CTP datasets from 14 different centers were included from the DUtch acute STroke (DUST) study. The AIF was taken as a direct measure to characterize contrast bolus injection. Statistical analysis was applied to evaluate differences in amplitude, area under the curve (AUC), bolus arrival time (BAT), and time to peak (TTP). To assess the clinical relevance of differences in AIF, CTP acquisitions were simulated with a realistic anthropomorphic digital phantom. Perfusion parameters were extracted by CTP analysis using commercial software (IntelliSpace Portal (ISP), version 10.1) as well as an in-house method based on block-circulant singular value decomposition (bSVD).
Results: A total of 1422 CTP datasets were included, ranging from 6 to 322 included patients per center. The measured values of the parameters used to characterize the AIF differed significantly with approximate interquartile ranges of 200-750 HU for the amplitude, 2500-10,000 HU·s for the AUC, 0-17 s for the BAT, and 10-26 s for the TTP. Mean infarct volumes of the phantom were significantly different between centers for both methods of perfusion analysis.
Conclusions: Although guidelines for the acquisition protocol are often provided for centers participating in a multicenter study, contrast medium injection protocols still vary. The resulting volumetric differences in infarct core and penumbra may impact clinical decision making in stroke diagnosis.
Key points: • The contrast medium injection protocol may be different between stroke centers participating in a harmonized multicenter study. • The contrast medium injection protocol influences the results of X-ray computed tomography perfusion imaging. • The contrast medium injection protocol can impact stroke diagnosis and patient selection for treatment.
Keywords: Contrast media; Perfusion imaging; Stroke; Tomography, X-ray computed.
© 2021. The Author(s).
Conflict of interest statement
The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article.
Figures




References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
