

Distinct immunological signatures discriminate severe COVID-19 from non-SARS-CoV-2-driven critical pneumonia
- PMID: 34051147
- PMCID: PMC8106882
- DOI: 10.1016/j.immuni.2021.05.002
Distinct immunological signatures discriminate severe COVID-19 from non-SARS-CoV-2-driven critical pneumonia
Erratum in
-
Distinct immunological signatures discriminate severe COVID-19 from non-SARS-CoV-2-driven critical pneumonia.Immunity. 2022 Feb 8;55(2):366-375. doi: 10.1016/j.immuni.2022.01.015. Immunity. 2022. PMID: 35139354 Free PMC article. No abstract available.
Abstract
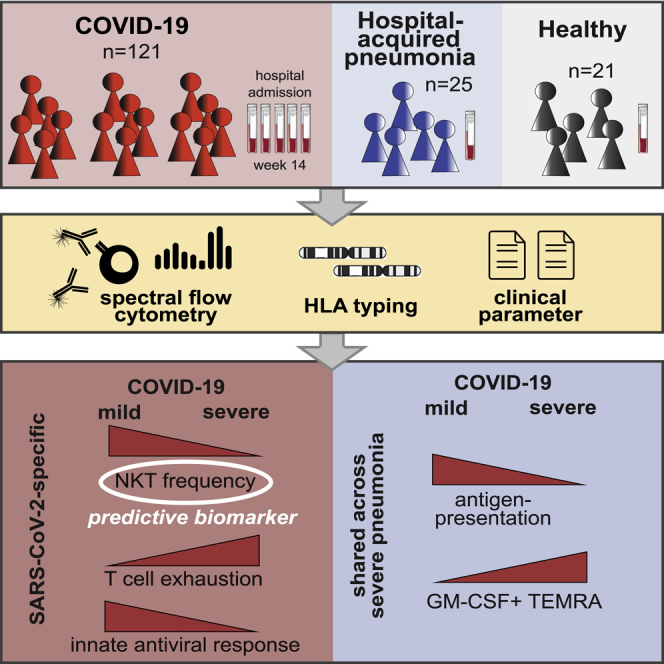
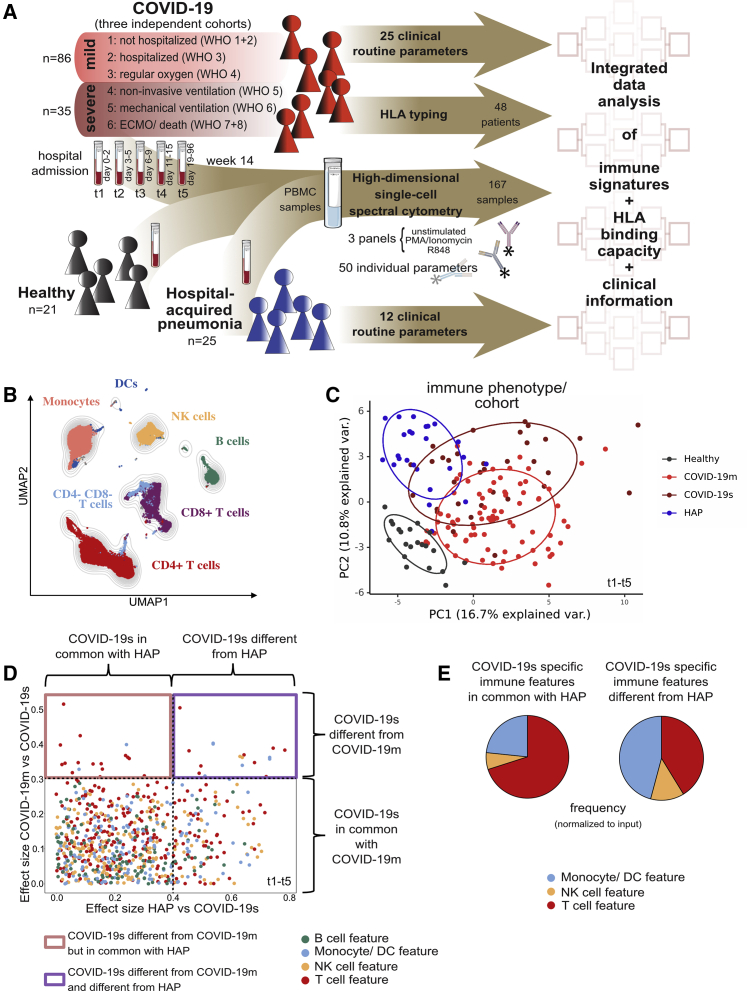
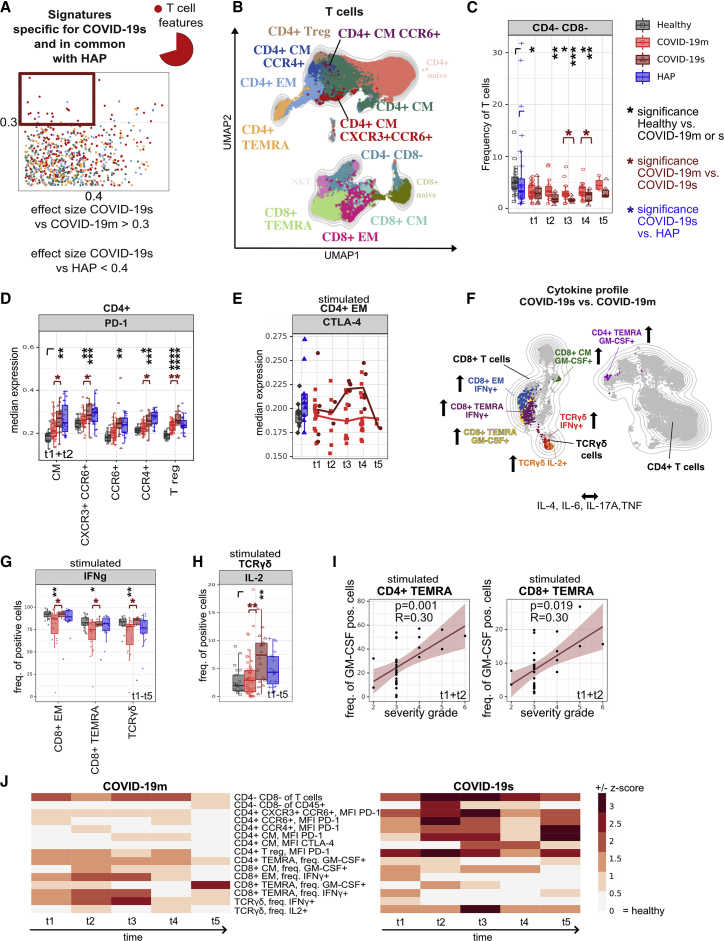
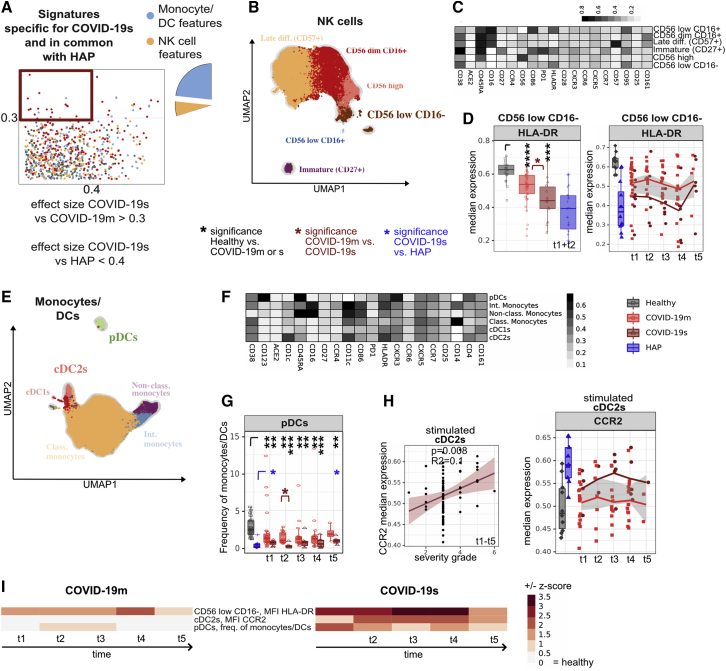
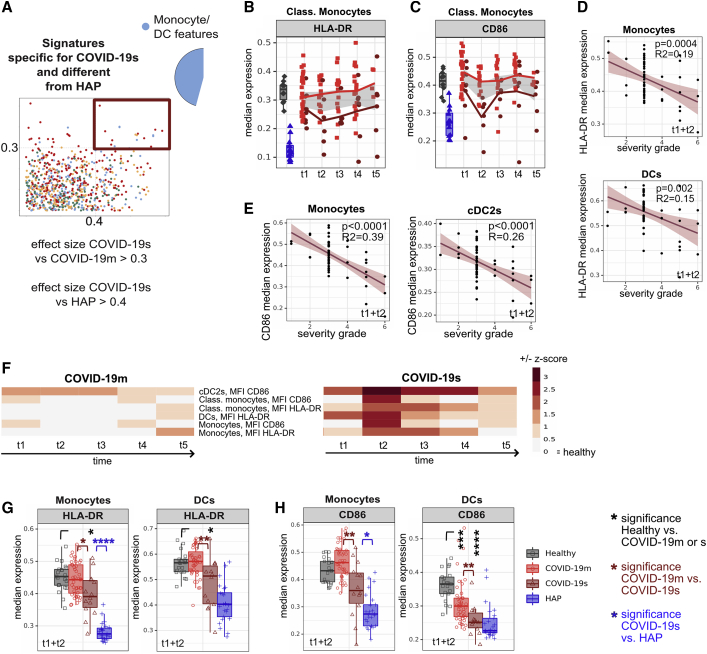
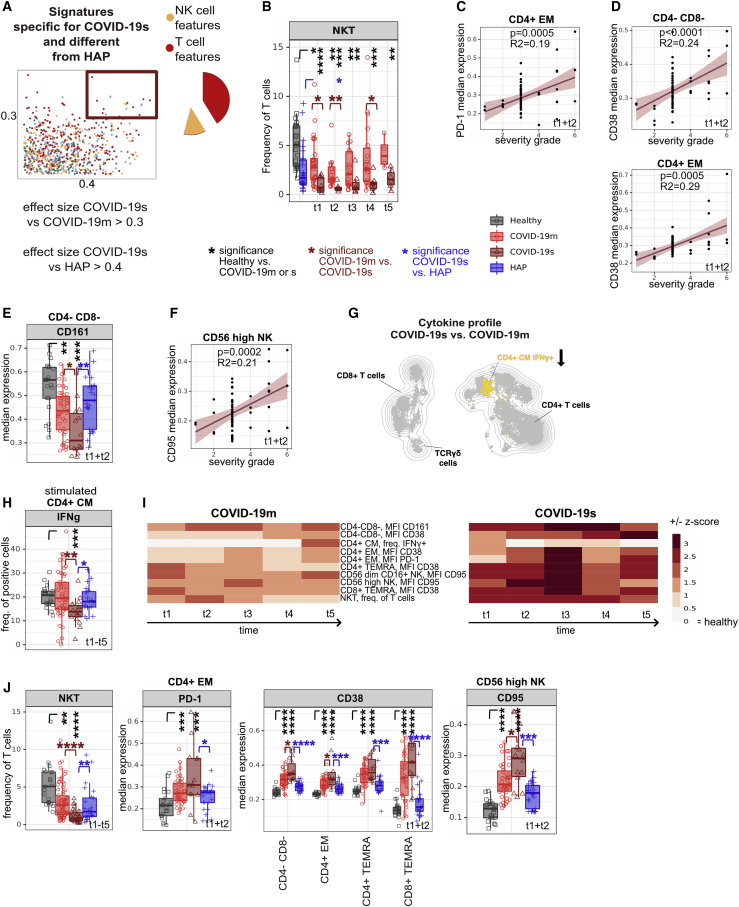
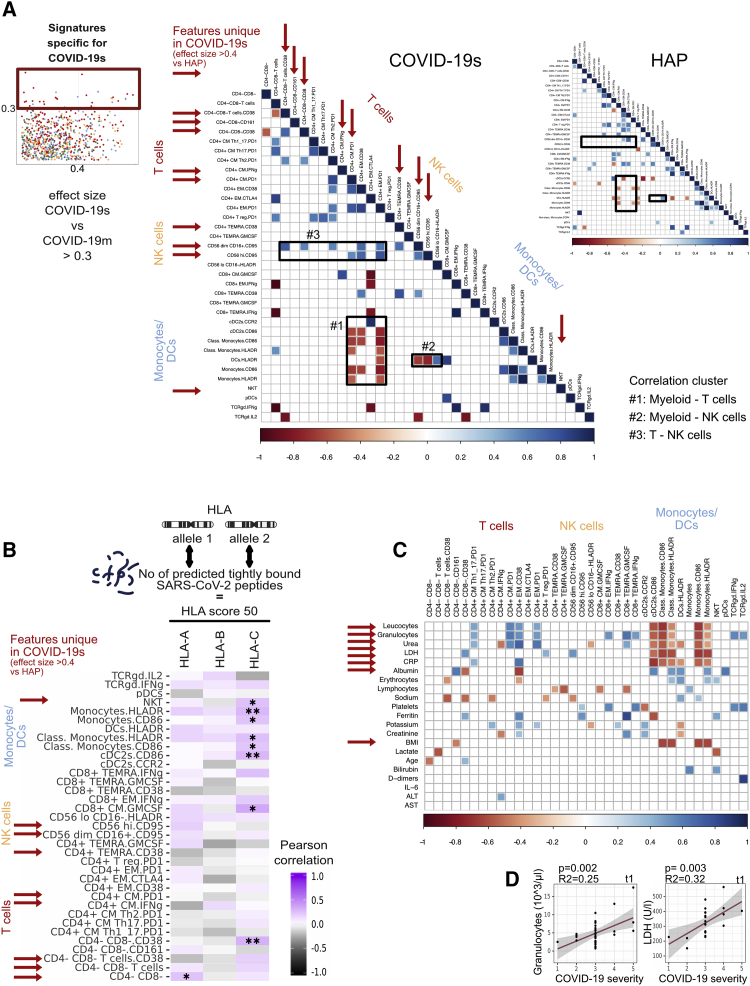
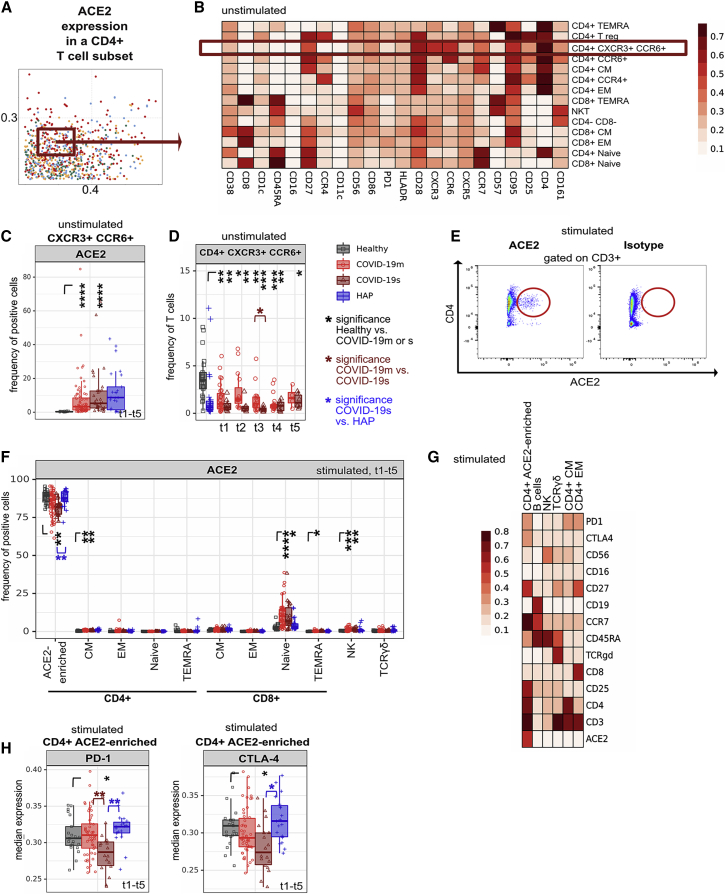
Immune profiling of COVID-19 patients has identified numerous alterations in both innate and adaptive immunity. However, whether those changes are specific to SARS-CoV-2 or driven by a general inflammatory response shared across severely ill pneumonia patients remains unknown. Here, we compared the immune profile of severe COVID-19 with non-SARS-CoV-2 pneumonia ICU patients using longitudinal, high-dimensional single-cell spectral cytometry and algorithm-guided analysis. COVID-19 and non-SARS-CoV-2 pneumonia both showed increased emergency myelopoiesis and displayed features of adaptive immune paralysis. However, pathological immune signatures suggestive of T cell exhaustion were exclusive to COVID-19. The integration of single-cell profiling with a predicted binding capacity of SARS-CoV-2 peptides to the patients' HLA profile further linked the COVID-19 immunopathology to impaired virus recognition. Toward clinical translation, circulating NKT cell frequency was identified as a predictive biomarker for patient outcome. Our comparative immune map serves to delineate treatment strategies to interfere with the immunopathologic cascade exclusive to severe COVID-19.
Trial registration: ClinicalTrials.gov NCT04385108.
Keywords: COVID-19; GM-CSF; HLA typing; SARS-CoV-2; biomarker; high-dimensional single cell analysis; immune profiling; immunophenotyping; peptide binding strength; spectral flow cytometry.
Copyright © 2021 The Author(s). Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests The authors declare no competing interests.
Figures
Comment in
-
Are NKT cells a useful predictor of COVID-19 severity?Immunity. 2022 Feb 8;55(2):185-187. doi: 10.1016/j.immuni.2022.01.005. Epub 2022 Jan 19. Immunity. 2022. PMID: 35104438 Free PMC article. No abstract available.
References
-
- Armstrong R.A., Kane A.D., Cook T.M. Outcomes from intensive care in patients with COVID-19: a systematic review and meta-analysis of observational studies. Anaesthesia. 2020;75:1340–1349. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
