

COVID-19-associated Aspergillus tracheobronchitis: the interplay between viral tropism, host defence, and fungal invasion
- PMID: 34051176
- PMCID: PMC8153840
- DOI: 10.1016/S2213-2600(21)00138-7
COVID-19-associated Aspergillus tracheobronchitis: the interplay between viral tropism, host defence, and fungal invasion
Abstract
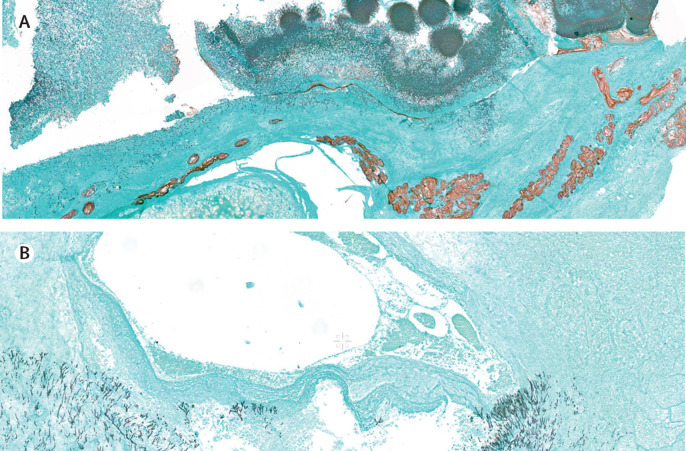
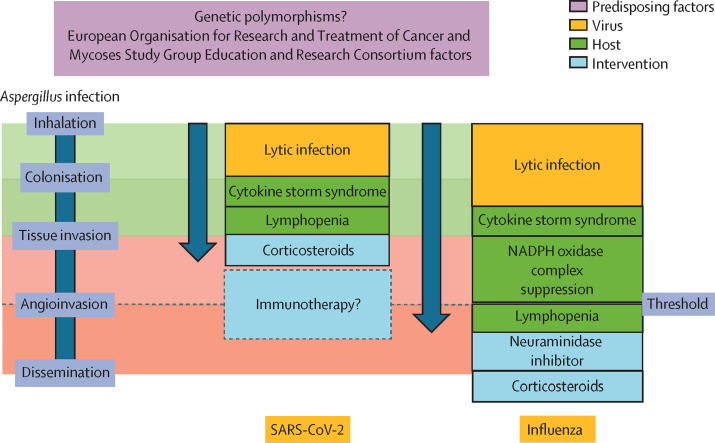
Invasive pulmonary aspergillosis is emerging as a secondary infection in patients with COVID-19, which can present as alveolar disease, airway disease (ie, invasive Aspergillus tracheobronchitis), or both. Histopathology of invasive Aspergillus tracheobronchitis in patients with severe COVID-19 confirms tracheal ulcers with tissue invasion of Aspergillus hyphae but without angioinvasion, which differs from patients with severe influenza, where early angioinvasion is observed. We argue that aggregation of predisposing factors (eg, factors that are defined by the European Organisation for Research and Treatment of Cancer and Mycoses Study Group Education and Research Consortium or genetic polymorphisms), viral factors (eg, tropism and lytic effects), immune defence factors, and effects of concomitant therapies will determine whether and when the angioinvasion threshold is reached. Management of invasive Aspergillus tracheobronchitis should include reducing viral lytic effects, rebalancing immune dysregulation, and systemic and local antifungal therapy. Future study designs should involve approaches that aim to develop improved diagnostics for tissue invasion and airways involvement and identify the immune status of the patient to guide personalised immunotherapy.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests RJMB reports grants from and consultancy for MSD, Pfizer, Mundipharma, F2G, Gilead Sciences, Astellas Pharma, and Amplyx Pharmaceuticals, outside of the submitted work. JW reports grants and personal fees from MSD, Gilead Sciences, and Pfizer during the study. PEV reports grants from Mundipharma, F2G, Pfizer, Thermo Fisher Scientific, Gilead Sciences, and Cidara Therapeutics and non-financial support from IMMY, outside of the submitted work. FLvdV reports personal fees from Gilead Sciences and Swedish Orphan Biovitrum, outside of the submitted work. SV, GDH, MHER, MGN, and JAS declare no competing interests.
Figures


References
-
- Schauwvlieghe AFAD, Rijnders BJA, Philips N, et al. Invasive aspergillosis in patients admitted to the intensive care unit with severe influenza: a retrospective cohort study. Lancet Respir Med. 2018;6:782–792. - PubMed
-
- van de Veerdonk FL, Kolwijck E, Lestrade PP, et al. Influenza-associated aspergillosis in critically ill patients. Am J Respir Crit Care Med. 2017;196:524–527. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
