

Deep learning for predicting COVID-19 malignant progression
- PMID: 34051438
- PMCID: PMC8112895
- DOI: 10.1016/j.media.2021.102096
Deep learning for predicting COVID-19 malignant progression
Abstract
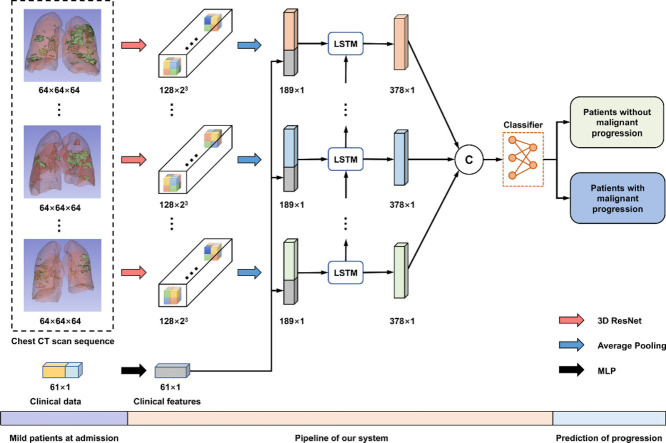
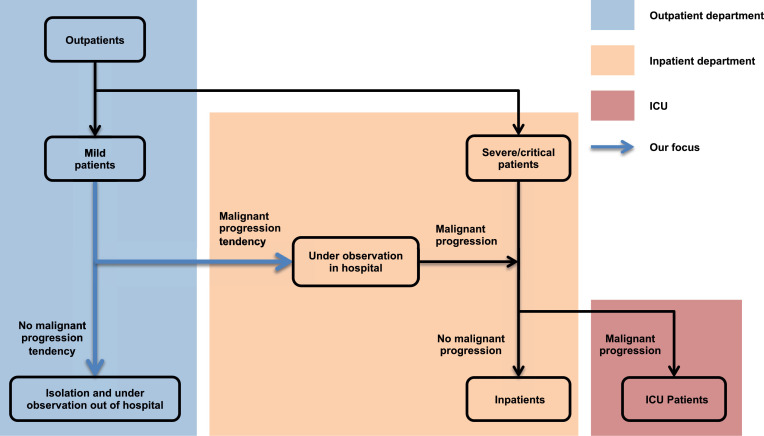
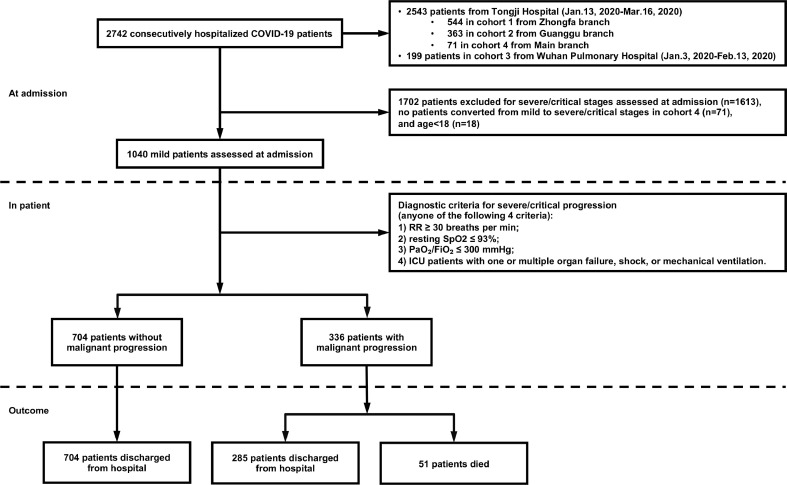
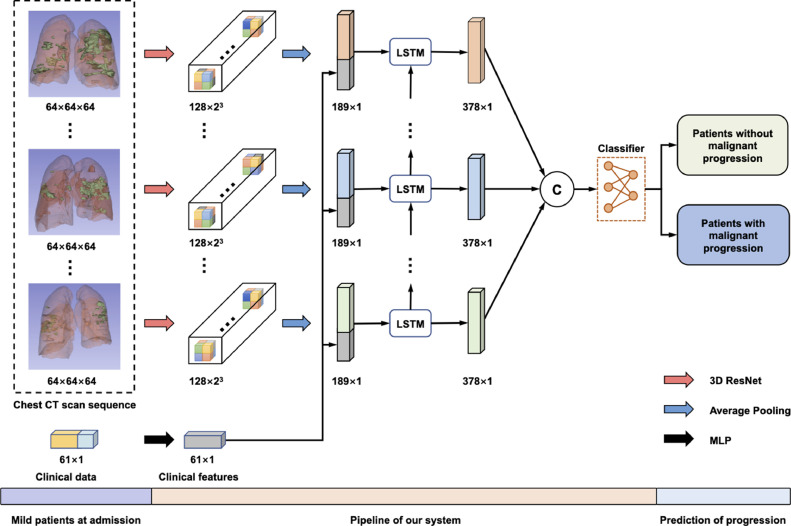
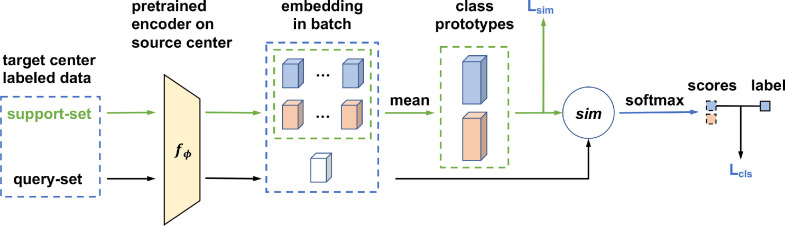
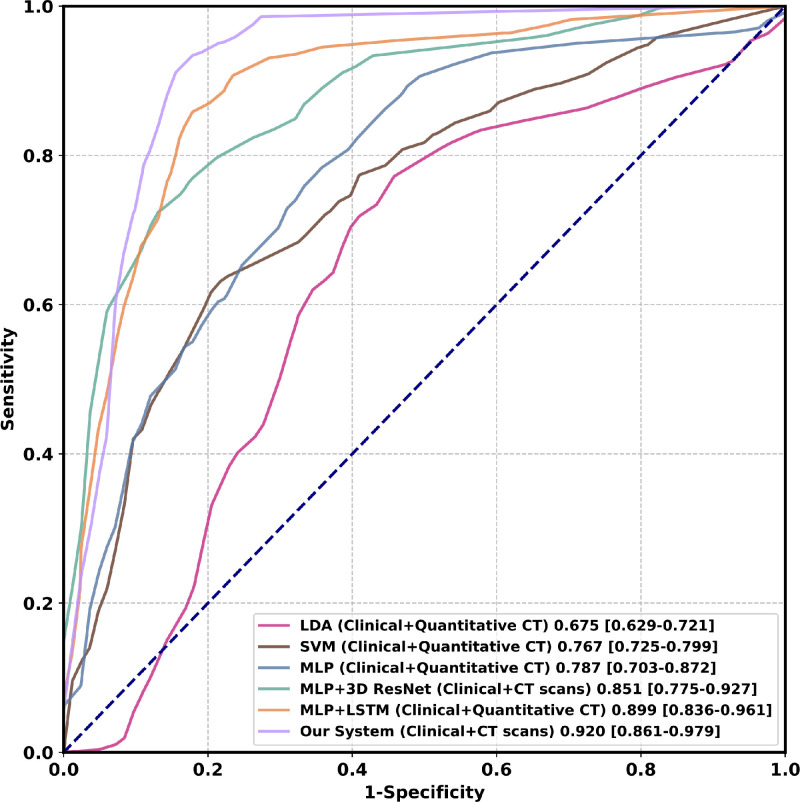
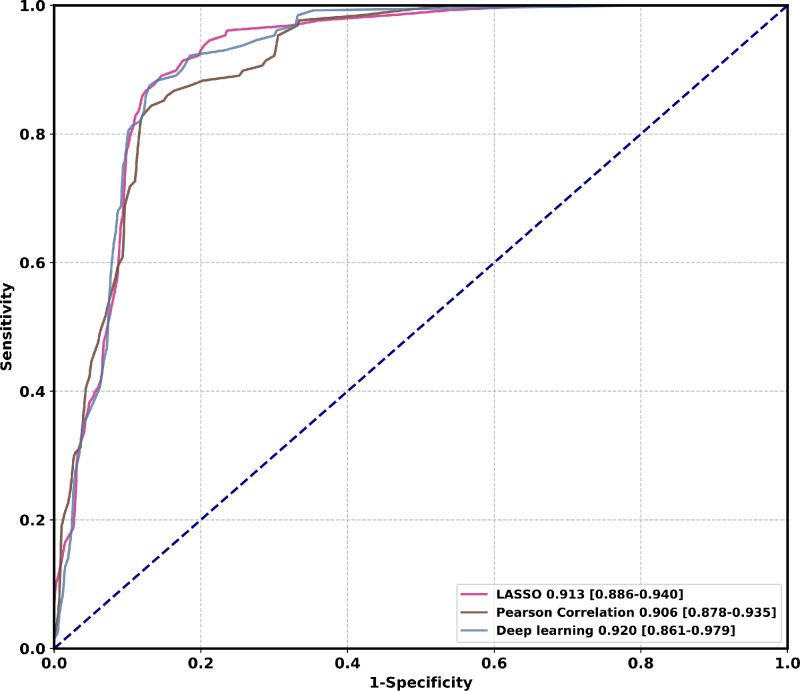
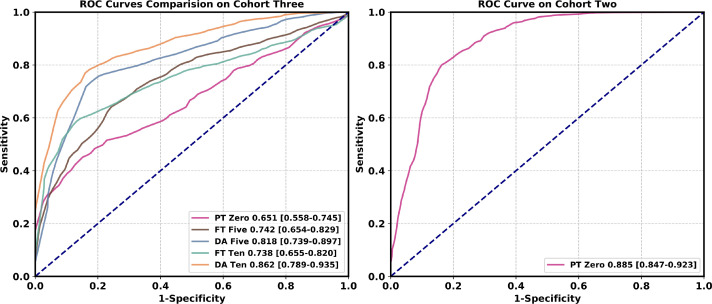
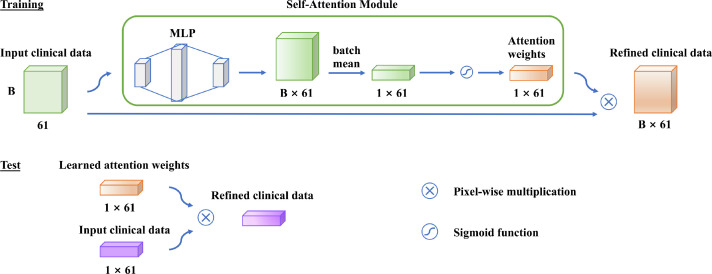
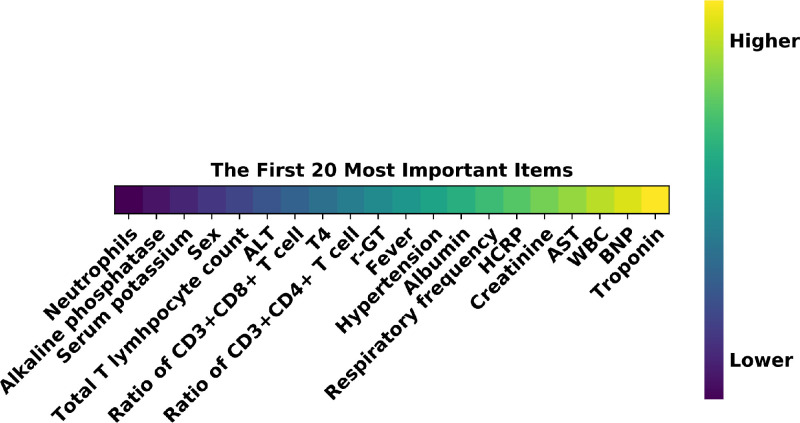
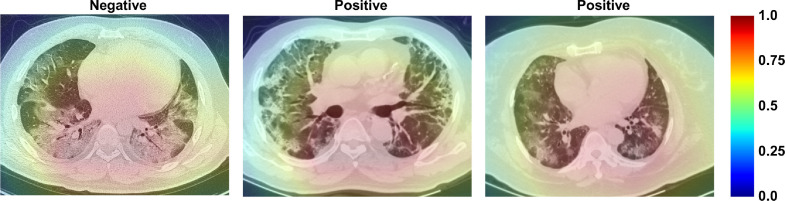
As COVID-19 is highly infectious, many patients can simultaneously flood into hospitals for diagnosis and treatment, which has greatly challenged public medical systems. Treatment priority is often determined by the symptom severity based on first assessment. However, clinical observation suggests that some patients with mild symptoms may quickly deteriorate. Hence, it is crucial to identify patient early deterioration to optimize treatment strategy. To this end, we develop an early-warning system with deep learning techniques to predict COVID-19 malignant progression. Our method leverages CT scans and the clinical data of outpatients and achieves an AUC of 0.920 in the single-center study. We also propose a domain adaptation approach to improve the generalization of our model and achieve an average AUC of 0.874 in the multicenter study. Moreover, our model automatically identifies crucial indicators that contribute to the malignant progression, including Troponin, Brain natriuretic peptide, White cell count, Aspartate aminotransferase, Creatinine, and Hypersensitive C-reactive protein.
Keywords: COVID-19; Domain adaptation; Feature fusion; Malignant progression.
Copyright © 2021 Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Bennhold K. A German exception? Why the country’s coronavirus death rate is low. New York Times. 2020;6(4):2020.
-
- Bermúdez-Chacón R., Becker C.J., Salzmann M., Fua P. MICCAI. 2016. Scalable unsupervised domain adaptation for electron microscopy. - PubMed
-
- Brown L., Cai T.T., DasGupta A. Interval estimation for a binomial proportion. Stat. Sci. 2001;16:101–133.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
