

Characterizing initiation, use, and discontinuation of extended-release buprenorphine in a nationally representative United States commercially insured cohort
- PMID: 34051547
- PMCID: PMC8488795
- DOI: 10.1016/j.drugalcdep.2021.108764
Characterizing initiation, use, and discontinuation of extended-release buprenorphine in a nationally representative United States commercially insured cohort
Abstract
Background and aims: While the United States is in the midst of an overdose epidemic, effective treatments are underutilized and commonly discontinued. Innovations in medication delivery, including an extended-release formulations, have the potential to improve treatment access and reduce discontinuation. We sought to assess extended-release buprenorphine discontinuation among individuals with opioid use disorder (OUD) in a real-world, nationally representative cohort.
Setting: United States PARTICIPANTS: Commercially insured individuals initiating one of four FDA-approved medications for opioid use disorder (MOUD) in 2018: extended-release buprenorphine, extended-release naltrexone, mucosal buprenorphine (mono- or co-formulated with naloxone), or methadone.
Measurements: Our primary outcome was medication discontinuation, defined as a gap of more than 14 days between the end of one prescription or administration and the subsequent dose.
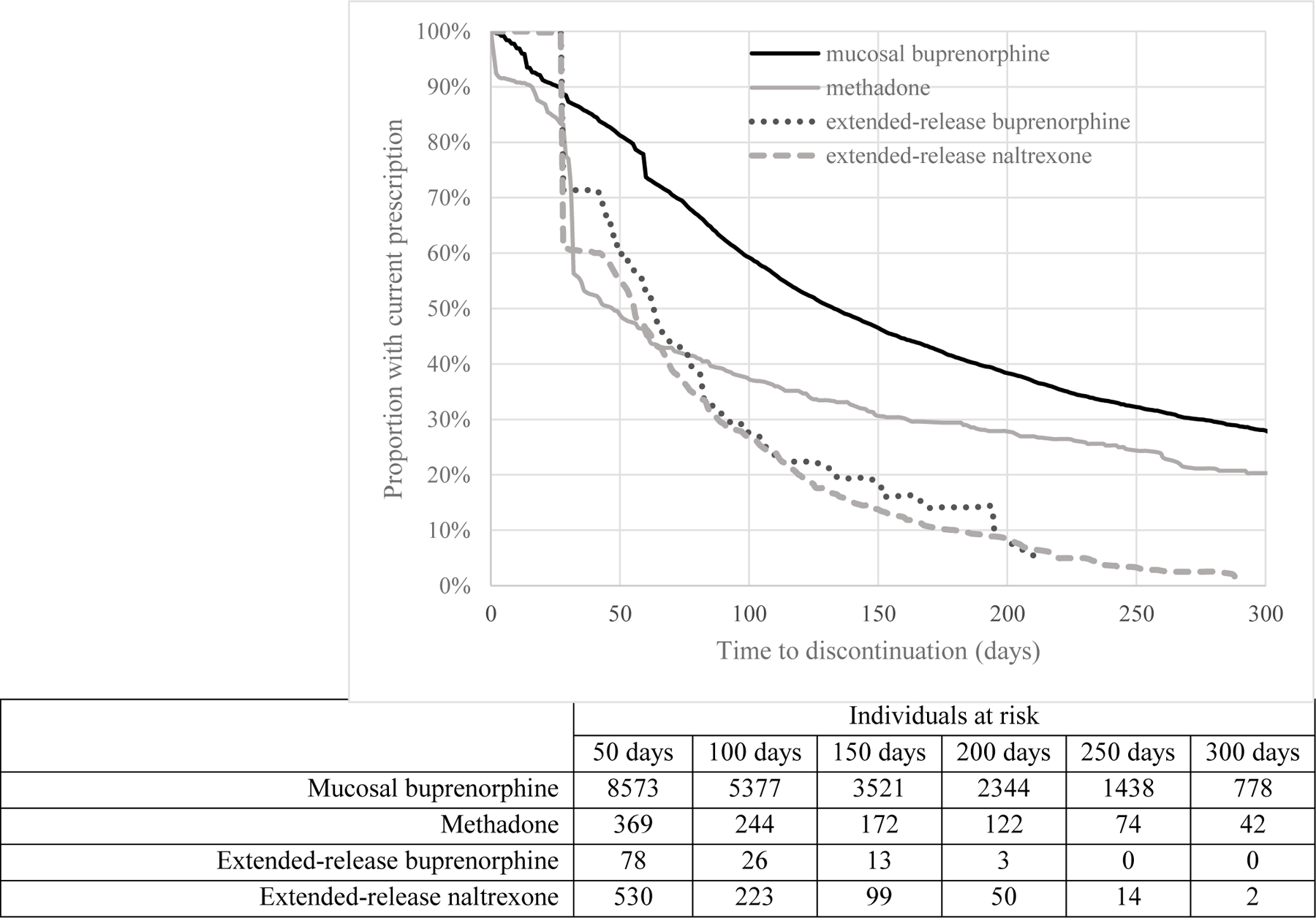
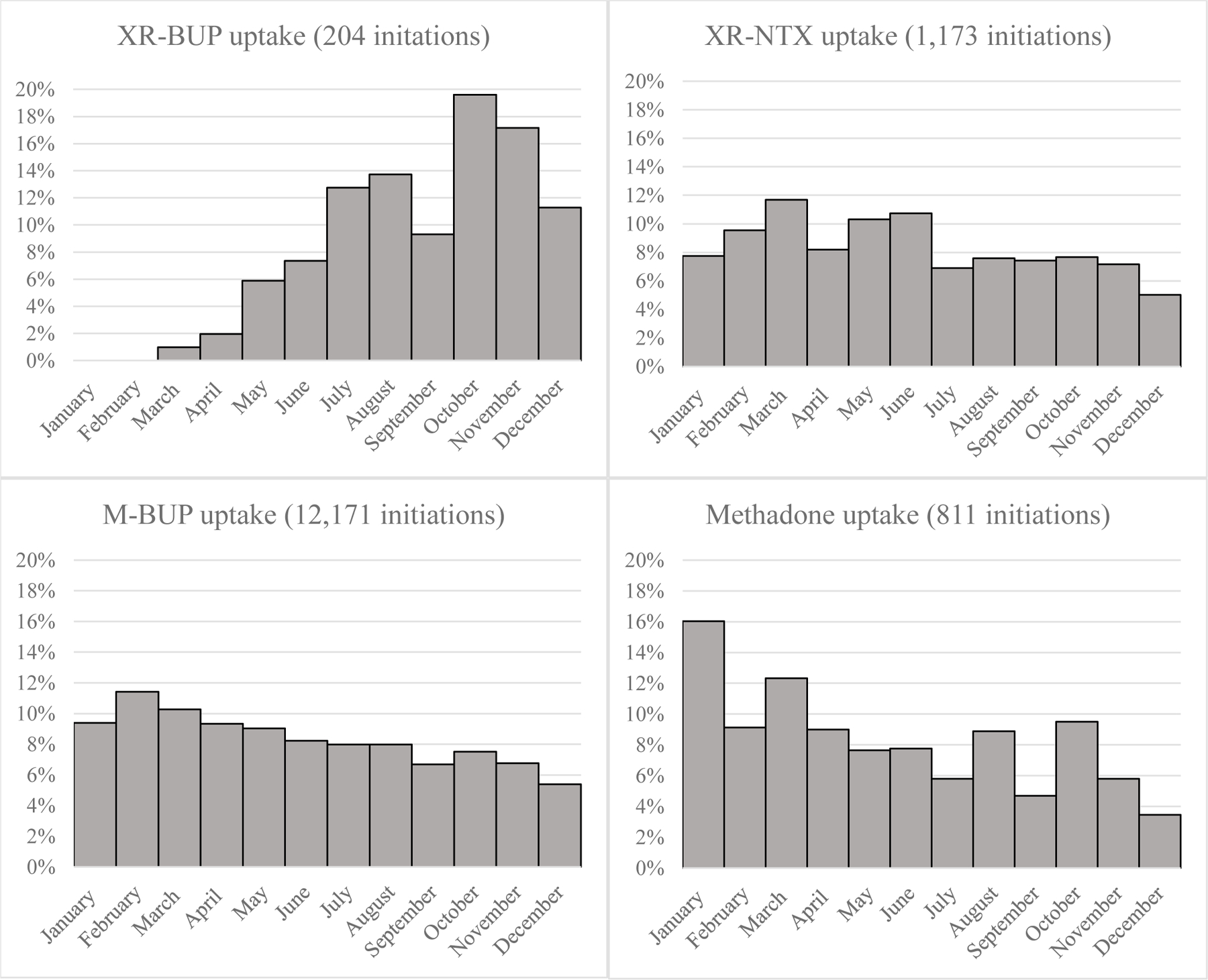
Findings: We identified 14,358 individuals initiating MOUD in 2018, including 204 (1%) extended-release buprenorphine, 1,173 (8%) extended-release naltrexone, 12,171 (85%) mucosal buprenorphine, and 810 (6%) methadone initiations. Three months after initiation, 50% (95% confidence interval [CI] 40%-60%) of extended-release buprenorphine, 64% (95% CI 61%-69%) of extended-release naltrexone, 34% (95% CI 33%-35%) of mucosal buprenorphine, and 58% (95% CI 54%-62%) of methadone initiators had discontinued treatment.
Conclusions: Across all treatment groups, medication discontinuation was high, and in this sample of early adopters with limited follow-up time, we found no evidence that extended-release buprenorphine offered a retention advantage compared to other MOUD in real-world settings. Retention continues to represent a major obstacle to treatment effectiveness, and interventions are needed to address this challenge even as new MOUD formulations become available.
Keywords: Extended-release buprenorphine; Medication for opioid Use disorder; Opioid use disorder; Retention.
Copyright © 2021 Elsevier B.V. All rights reserved.
Figures
Similar articles
-
Injectable naltrexone, oral naltrexone, and buprenorphine utilization and discontinuation among individuals treated for opioid use disorder in a United States commercially insured population.J Subst Abuse Treat. 2018 Feb;85:90-96. doi: 10.1016/j.jsat.2017.07.001. Epub 2017 Jul 3. J Subst Abuse Treat. 2018. PMID: 28733097 Free PMC article.
-
Medications for opioid use disorder: Predictors of early discontinuation and reduction of overdose risk in US military veterans by medication type.Addiction. 2025 Jan;120(1):138-151. doi: 10.1111/add.16659. Epub 2024 Sep 7. Addiction. 2025. PMID: 39243190 Free PMC article.
-
Examining differences in retention on medication for opioid use disorder: An analysis of Ohio Medicaid data.J Subst Abuse Treat. 2022 May;136:108686. doi: 10.1016/j.jsat.2021.108686. Epub 2021 Dec 15. J Subst Abuse Treat. 2022. PMID: 34953637
-
Prior National Drug Abuse Treatment Clinical Trials Network (CTN) opioid use disorder trials as background and rationale for NIDA CTN-0100 "optimizing retention, duration and discontinuation strategies for opioid use disorder pharmacotherapy (RDD)".Addict Sci Clin Pract. 2021 Mar 6;16(1):15. doi: 10.1186/s13722-021-00223-z. Addict Sci Clin Pract. 2021. PMID: 33676577 Free PMC article. Review.
-
Maintenance medication for opiate addiction: the foundation of recovery.J Addict Dis. 2012;31(3):207-25. doi: 10.1080/10550887.2012.694598. J Addict Dis. 2012. PMID: 22873183 Free PMC article. Review.
Cited by
-
Cannabidiol Effect on Cue-Induced Craving for Individuals with Opioid Use Disorder Treated with Buprenorphine: A Small Proof-of-Concept Open-Label Study.Integr Med Rep. 2022 Aug 1;1(1):157-163. doi: 10.1089/imr.2022.0070. Epub 2022 Aug 26. Integr Med Rep. 2022. PMID: 36105269 Free PMC article.
-
Impact of cannabidiol on reward- and stress-related neurocognitive processes among individuals with opioid use disorder: A pilot, double-blind, placebo-controlled, randomized cross-over trial.Front Psychiatry. 2023 Mar 30;14:1155984. doi: 10.3389/fpsyt.2023.1155984. eCollection 2023. Front Psychiatry. 2023. PMID: 37065899 Free PMC article.
-
Characterizing the Association Between Traumatic Brain Injury and Discontinuation of Medications for Opioid Use Disorder in a Commercially Insured Adult Population.J Head Trauma Rehabil. 2025 Mar-Apr 01;40(2):E111-E120. doi: 10.1097/HTR.0000000000000964. Epub 2024 Jun 27. J Head Trauma Rehabil. 2025. PMID: 39019485
-
Retention and dropout from sublingual and extended-release buprenorphine treatment: A comparative analysis of data from a nationally representative sample of commercially-insured people with opioid use disorder in the United States.Int J Drug Policy. 2025 Apr;138:104748. doi: 10.1016/j.drugpo.2025.104748. Epub 2025 Feb 27. Int J Drug Policy. 2025. PMID: 40020306 Free PMC article.
-
Barriers to accessing medications for opioid use disorder among rural individuals.Int J Drug Policy. 2025 Jun;140:104805. doi: 10.1016/j.drugpo.2025.104805. Epub 2025 Apr 19. Int J Drug Policy. 2025. PMID: 40252371
References
-
- Gladden RM, Martinez P, Seth P. Fentanyl Law Enforcement Submissions and Increases in Synthetic Opioid-Involved Overdose Deaths - 27 States, 2013–2014. MMWR Morb Mortal Wkly Rep 2016;65:837–43. - PubMed
-
- Davenport S, Matthews K. Opioid use disorder in the United States: Diagnosed prevalence by payer, age, sex, and state Washington, DC: Milliman; 2018.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
