

Pulmonary Nocardia infection in a child with idiopathic pulmonary hemosiderosis
- PMID: 34051779
- PMCID: PMC8164755
- DOI: 10.1186/s12890-021-01544-0
Pulmonary Nocardia infection in a child with idiopathic pulmonary hemosiderosis
Abstract
Background: Idiopathic pulmonary hemosiderosis (IPH) encompasses a rare and agnogenic group of diffuse alveolar capillary hemorrhagic diseases. Corticosteroid treatment is the globally preferred therapeutic strategy for IPH; however, it can cause immunodeficiency. Nocardia infection often occurs in immunocompromised patients and primarily involves the pleura and lungs. Herein, we describe a case of pediatric pulmonary Nocardia infection after the corticosteroid treatment of IPH.
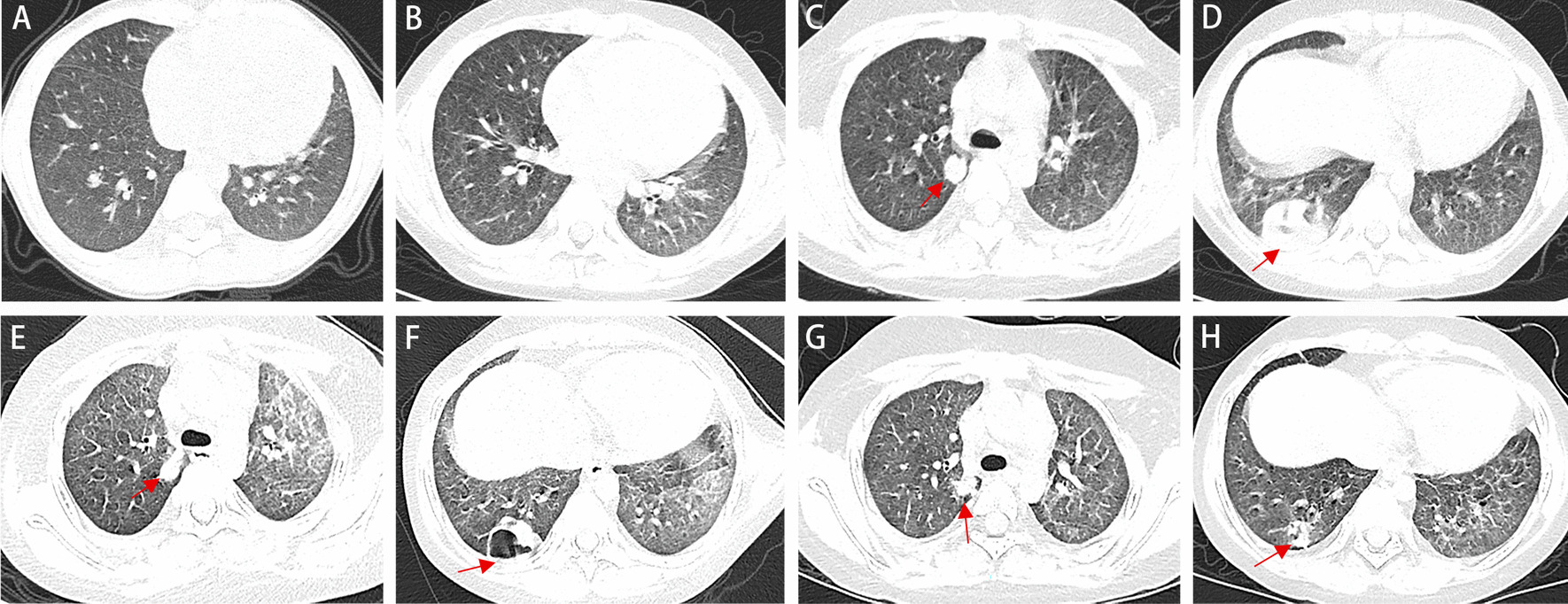
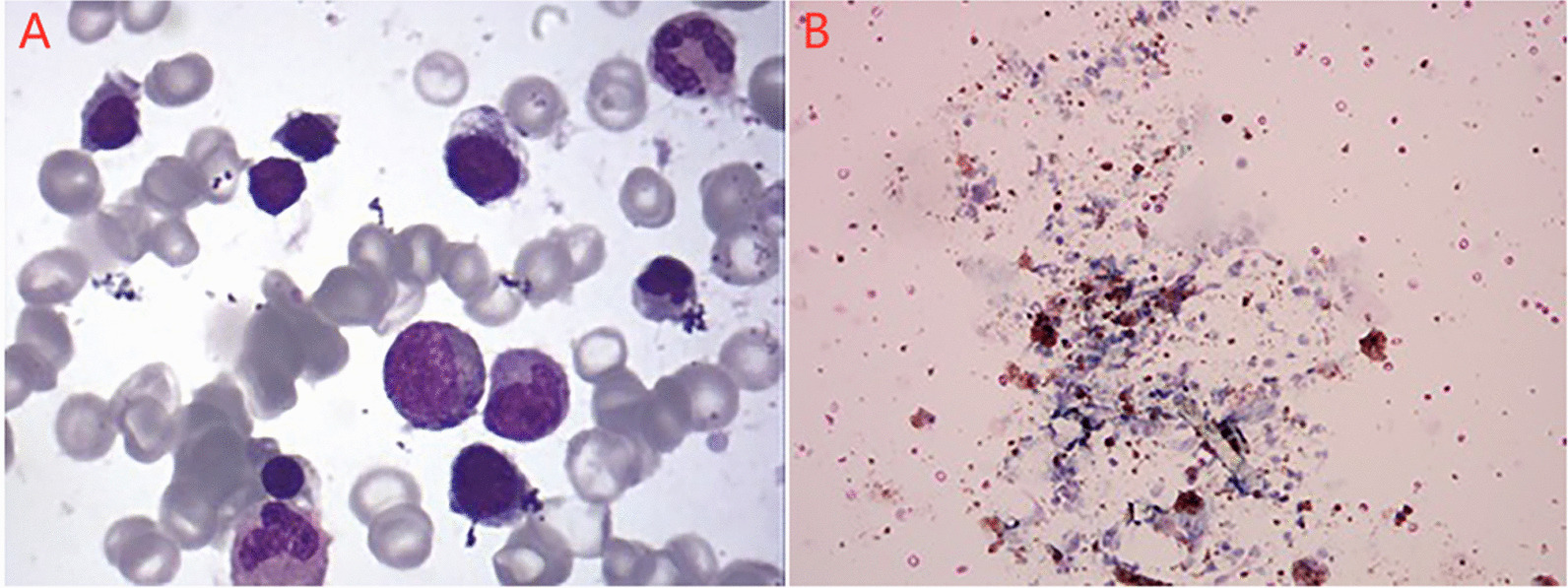
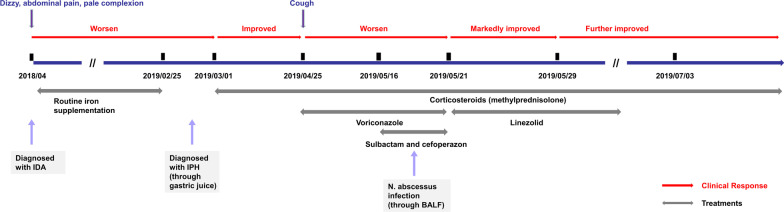
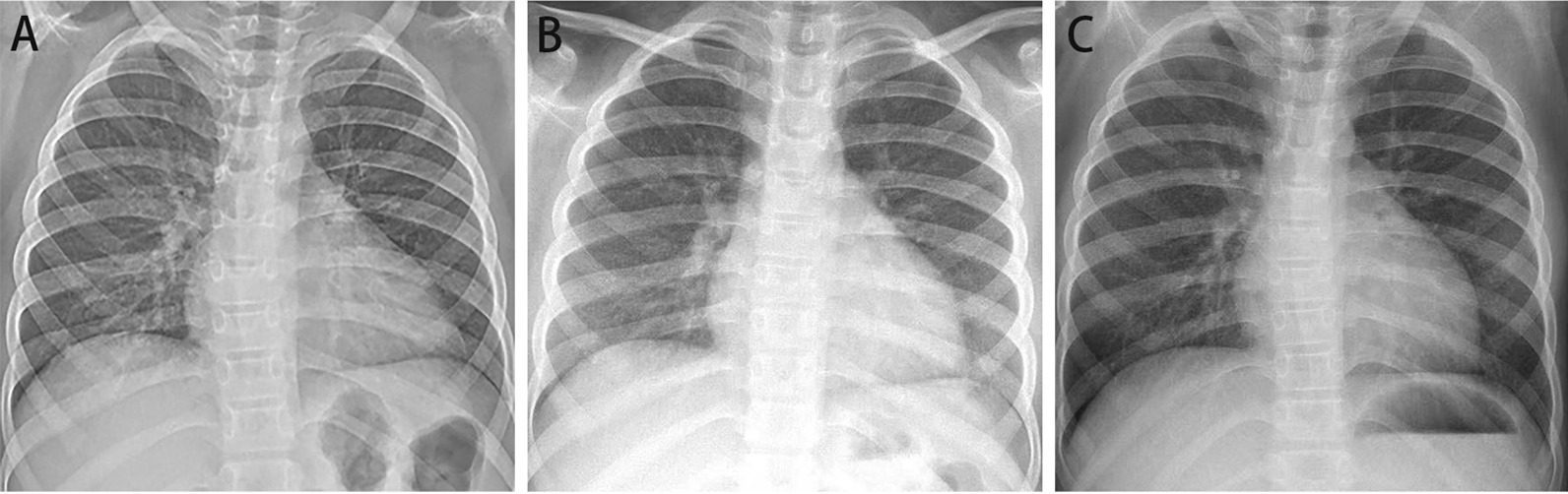
Case presentation: A 7-year-old girl presented with chief complaints of pale complexion persisting for 1 year and a cough for 20 days. Abundant hemosiderin-laden macrophages were detected in the gastric juice, which supported the diagnosis of IPH. Uninterrupted doses of corticosteroids were administered during the last hospitalization. After nearly 2 months of corticosteroids therapy, the patient began to cough and produce a purulent sputum. Next-generation sequencing of the bronchoalveolar lavage fluid revealed Nocardia abscessus (N. abscessus) DNA. Linezolid was administered with good response, and the patient was discharged after 18 days of hospitalization. Her symptoms and pulmonary lesions had recovered, and the IPH appeared to be well-controlled with low dose of corticosteroids in follow-up.
Conclusions: Nocardia infection should be considered in the differential diagnoses for IPH patients receiving corticosteroid therapy, especially in patients with poor response to conventional empirical antibiotic therapy. Next-generation sequencing of bronchoalveolar lavage fluid may be used to quickly identify the Nocardia. Sulfonamides or linezolid are effective for pediatric pulmonary Nocardia infection.
Keywords: Corticosteroid; Hemosiderin-laden macrophages; Idiopathic; Nocardia; Pulmonary hemosiderosis.
Conflict of interest statement
There is no any competing interest.
Figures
Similar articles
-
Anemia as the sole presenting symptom of idiopathic pulmonary hemosiderosis: report of two cases.Chang Gung Med J. 2004 Nov;27(11):824-9. Chang Gung Med J. 2004. PMID: 15796258
-
A Case of Idiopathic Pulmonary Hemosiderosis Presenting With Signs and Symptoms Mimicking Hemolytic Anemia.J Pediatr Hematol Oncol. 2017 Jan;39(1):e15-e17. doi: 10.1097/MPH.0000000000000722. J Pediatr Hematol Oncol. 2017. PMID: 27918350
-
Idiopathic pulmonary hemosiderosis in a child: report of one case.Acta Paediatr Taiwan. 2001 Mar-Apr;42(2):101-4. Acta Paediatr Taiwan. 2001. PMID: 11355061
-
Idiopathic pulmonary hemosiderosis: A state of the art review.Respir Med. 2021 Jan;176:106234. doi: 10.1016/j.rmed.2020.106234. Epub 2020 Nov 17. Respir Med. 2021. PMID: 33246295 Review.
-
Updates in idiopathic pulmonary hemosiderosis in 2022: A state of the art review.Pediatr Pulmonol. 2023 Feb;58(2):382-391. doi: 10.1002/ppul.26230. Epub 2022 Nov 11. Pediatr Pulmonol. 2023. PMID: 36324124 Review.
Cited by
-
Nocardia farcinica pneumonia complicated by pneumocystis jiroveci infection in children with Neuromyelitis Optica Spectrum Disorders: a case report and literature review.Ital J Pediatr. 2024 Dec 2;50(1):255. doi: 10.1186/s13052-024-01827-2. Ital J Pediatr. 2024. PMID: 39617880 Free PMC article. Review.
-
Unusual presentation of Nocardia abscessus infection in an immunocompetent patient.Access Microbiol. 2022 Feb 2;4(2):000308. doi: 10.1099/acmi.0.000308. eCollection 2022. Access Microbiol. 2022. PMID: 35355873 Free PMC article.
-
Pneumonia Caused by Coinfection with Cytomegalovirus and Pneumocystis jirovecii in an HIV-Negative Infant Diagnosed by Metagenomic Next-Generation Sequencing.Infect Drug Resist. 2022 Jun 30;15:3417-3425. doi: 10.2147/IDR.S364241. eCollection 2022. Infect Drug Resist. 2022. PMID: 35800120 Free PMC article.
-
A rare case of pulmonary nocardiosis comorbid with Sjogren's syndrome.J Clin Lab Anal. 2021 Sep;35(9):e23902. doi: 10.1002/jcla.23902. Epub 2021 Aug 21. J Clin Lab Anal. 2021. PMID: 34418167 Free PMC article.
References
-
- Kiper N, Göçmen A, Özçelik U, Dilber E, Anadol D. Long-term clinical course of patients with idiopathic pulmonary hemosiderosis (1979–1994): prolonged survival with low-dose corticosteroid therapy. Pediatr Pulmonol. 1999;27(3):180–184. doi: 10.1002/(sici)1099-0496(199903)27:3<180::aid-ppul5>3.0.co;2-8. - DOI - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
