

Spatial, temporal, and demographic patterns in prevalence of chewing tobacco use in 204 countries and territories, 1990-2019: a systematic analysis from the Global Burden of Disease Study 2019
- PMID: 34051920
- PMCID: PMC8251505
- DOI: 10.1016/S2468-2667(21)00065-7
Spatial, temporal, and demographic patterns in prevalence of chewing tobacco use in 204 countries and territories, 1990-2019: a systematic analysis from the Global Burden of Disease Study 2019
Erratum in
-
Correction to Lancet Public Health 2021; published online May 27. https://doi.org/10.1016/S2468-2667(21)00065-7.Lancet Public Health. 2021 Jul;6(7):e449. doi: 10.1016/S2468-2667(21)00132-8. Epub 2021 Jun 3. Lancet Public Health. 2021. PMID: 34089663 Free PMC article. No abstract available.
Abstract
Background: Chewing tobacco and other types of smokeless tobacco use have had less attention from the global health community than smoked tobacco use. However, the practice is popular in many parts of the world and has been linked to several adverse health outcomes. Understanding trends in prevalence with age, over time, and by location and sex is important for policy setting and in relation to monitoring and assessing commitment to the WHO Framework Convention on Tobacco Control.
Methods: We estimated prevalence of chewing tobacco use as part of the Global Burden of Diseases, Injuries, and Risk Factors Study 2019 using a modelling strategy that used information on multiple types of smokeless tobacco products. We generated a time series of prevalence of chewing tobacco use among individuals aged 15 years and older from 1990 to 2019 in 204 countries and territories, including age-sex specific estimates. We also compared these trends to those of smoked tobacco over the same time period.
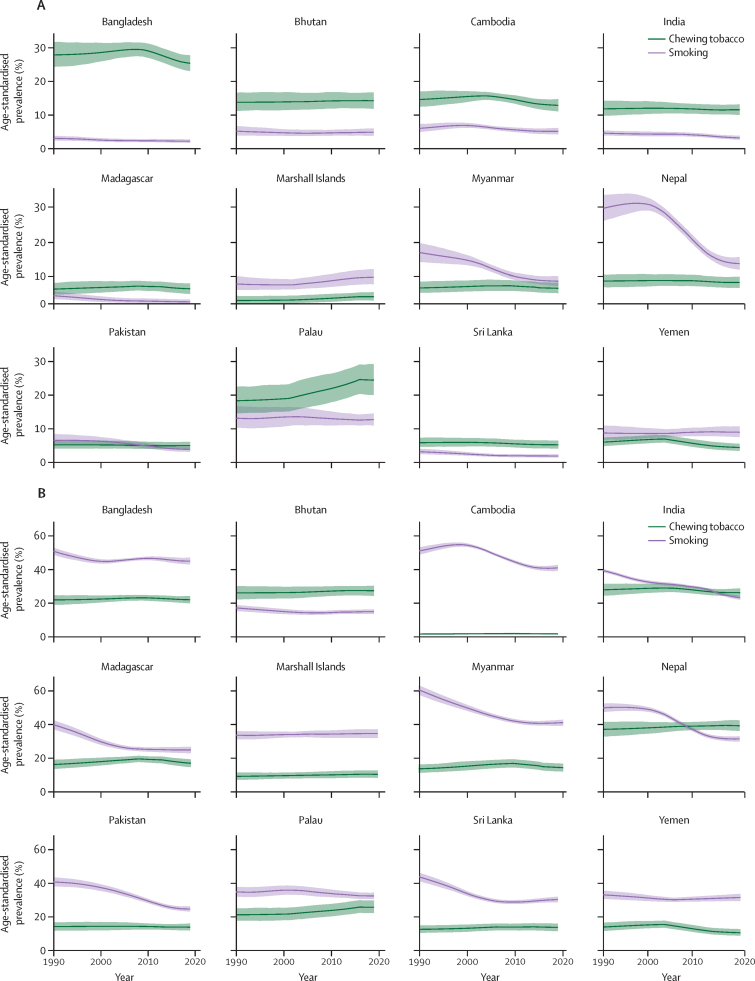
Findings: In 2019, 273·9 million (95% uncertainty interval 258·5 to 290·9) people aged 15 years and older used chewing tobacco, and the global age-standardised prevalence of chewing tobacco use was 4·72% (4·46 to 5·01). 228·2 million (213·6 to 244·7; 83·29% [82·15 to 84·42]) chewing tobacco users lived in the south Asia region. Prevalence among young people aged 15-19 years was over 10% in seven locations in 2019. Although global age-standardised prevalence of smoking tobacco use decreased significantly between 1990 and 2019 (annualised rate of change: -1·21% [-1·26 to -1·16]), similar progress was not observed for chewing tobacco (0·46% [0·13 to 0·79]). Among the 12 highest prevalence countries (Bangladesh, Bhutan, Cambodia, India, Madagascar, Marshall Islands, Myanmar, Nepal, Pakistan, Palau, Sri Lanka, and Yemen), only Yemen had a significant decrease in the prevalence of chewing tobacco use, which was among males between 1990 and 2019 (-0·94% [-1·72 to -0·14]), compared with nine of 12 countries that had significant decreases in the prevalence of smoking tobacco. Among females, none of these 12 countries had significant decreases in prevalence of chewing tobacco use, whereas seven of 12 countries had a significant decrease in the prevalence of tobacco smoking use for the period.
Interpretation: Chewing tobacco remains a substantial public health problem in several regions of the world, and predominantly in south Asia. We found little change in the prevalence of chewing tobacco use between 1990 and 2019, and that control efforts have had much larger effects on the prevalence of smoking tobacco use than on chewing tobacco use in some countries. Mitigating the health effects of chewing tobacco requires stronger regulations and policies that specifically target use of chewing tobacco, especially in countries with high prevalence.
Funding: Bloomberg Philanthropies and the Bill & Melinda Gates Foundation.
Copyright © 2021 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests ViA reports personal fees from Bayer Healthcare, Boehringer Ingelheim/Lilly alliance, Bristol Myers Squibb/Pfizer alliance, and Novo Nordisk outside of the submitted work. RA reports consultancy and speakers' fees from UCB, Sandoz, AbbVie, Zentiva, Teva, Laropharm, Cegedim, Angelini, B Braun, Biessen Pharma, Hofigal, AstraZeneca, and Stada. BA reports personal fees from Australian Institute of Sports, grants and non-financial support from Natural Remedies, and non-financial support from Zydus Cadila outside of the submitted work. SI reports grants from National Heart Foundation of Australia, and Australian National Health and Medical Research Council outside the submitted work. KK reports non-financial support from UGC Centre of Advanced Study (CAS II), Department of Anthropology, Panjab University, Chandigarh, India, outside of the submitted work. TRM reports contracts from Gov't Plaintiff Lawyers, JUUL, outside of the submitted work. JAS reports consultancy fees from Crealta/Horizon, Medisys, Fidia, Two Labs Inc, Adept Field Solutions, Clinical Care Options, Clearview Healthcare Partners, Putnam Associates, Focus Forward, Navigant Consulting, Spherix, MedIQ, UBM LLC, Trio Health, Medscape, WebMD, Practice Point Communications, and the National Institutes of Health and the American College of Rheumatology; receives payment for lectures as a member on the speaker's bureau of Simply Speaking; owns stock options in TPT Global Tech, Vaxart pharmaceuticals, and Charlotte's Web Holdings; previously owned stock options in Amarin, Viking, and Moderna pharmaceuticals; held a placement on the steering committee of OMERACT, an international organisation that develops measures for clinical trials and receives arm's length funding from 12 pharmaceutical companies; serves on the US Food and Drug Administration Arthritis Advisory Committee; is a member of the Veterans Affairs Rheumatology Field Advisory Committee; is the editor and is the Director of the University of Alabama at Birmingham Cochrane Musculoskeletal Group Satellite Center on Network Meta-analysis, all outside of the submitted work. JS reports ownership of companies providing services to Itrim, Amgen, Janssen, Novo Nordisk, Eli Lilly, Boehringer Ingelheim, Bayer, Pfizer, and AstraZeneca outside of the submitted work. DJS reports personal fees from Lundbeck, Takeda, Johnson & Johnson, and Servier outside of the submitted work. SS reports grants from Edwards Lifesciences, Medtronic, Boston Scientific, and Abbott; and personal fees from Boston Scientific, Teleflex, and BTG outside of the submitted work. All other authors declare no competing interests.
Figures


References
-
- Giovino GA, Biener L, Hartman AM. Monitoring the tobacco use epidemic I. Overview: optimizing measurement to facilitate change. Prev Med. 2009;48(suppl):S4–10. - PubMed
-
- Mehrotra R, Yadav A, Sinha DN. Smokeless tobacco control in 180 countries across the globe: call to action for full implementation of WHO FCTC measures. Lancet Oncol. 2019;20:e208–e217. - PubMed
-
- Palipudi K, Rizwan SA, Sinha DN. Prevalence and sociodemographic determinants of tobacco use in four countries of the World Health Organization: South-East Asia region: findings from the Global Adult Tobacco Survey. Indian J Cancer. 2014;51(suppl 1):S24–S32. - PubMed
-
- Sinha DN, Rizwan SA, Aryal KK, Karki KB, Zaman MM, Gupta PC. Trends of smokeless tobacco use among adults (aged 15–49 years) in Bangladesh, India and Nepal. Asian Pac J Cancer Prev. 2015;16:6561–6568. - PubMed
-
- Sinha DN, Kumar A, Bhartiya D. Smokeless tobacco use among adolescents in global perspective. Nicotine Tob Res. 2017;19:1395–1396. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
