

The impact of school reopening on the spread of COVID-19 in England
- PMID: 34053259
- PMCID: PMC8165595
- DOI: 10.1098/rstb.2020.0261
The impact of school reopening on the spread of COVID-19 in England
Abstract
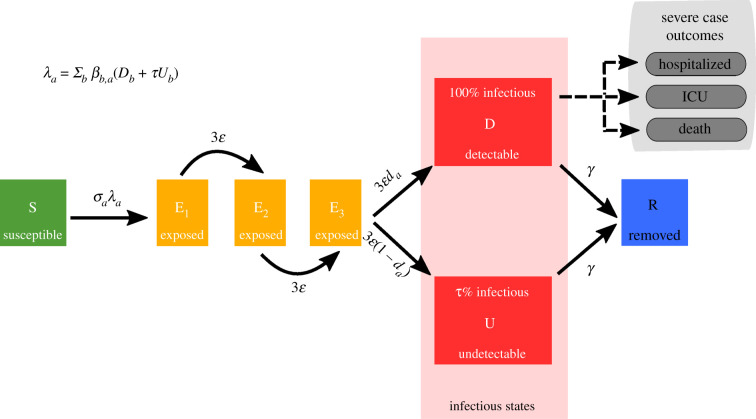
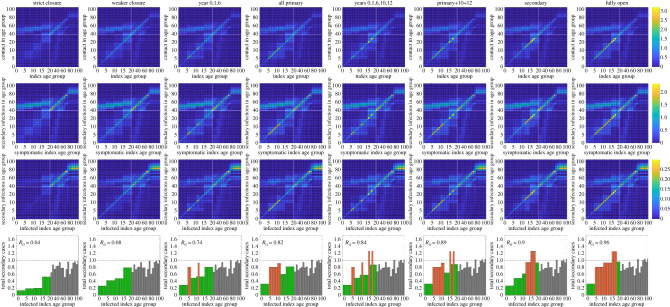
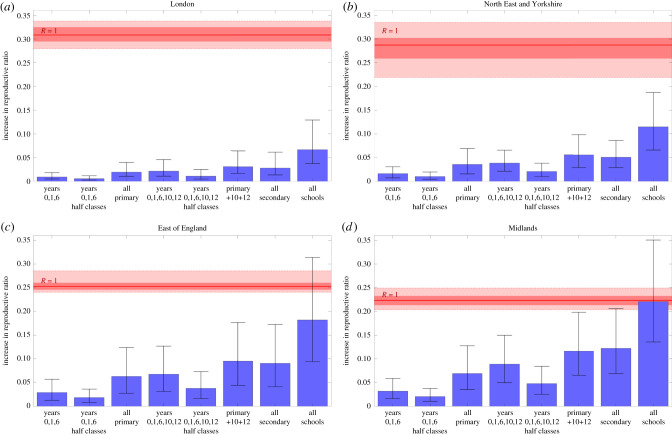
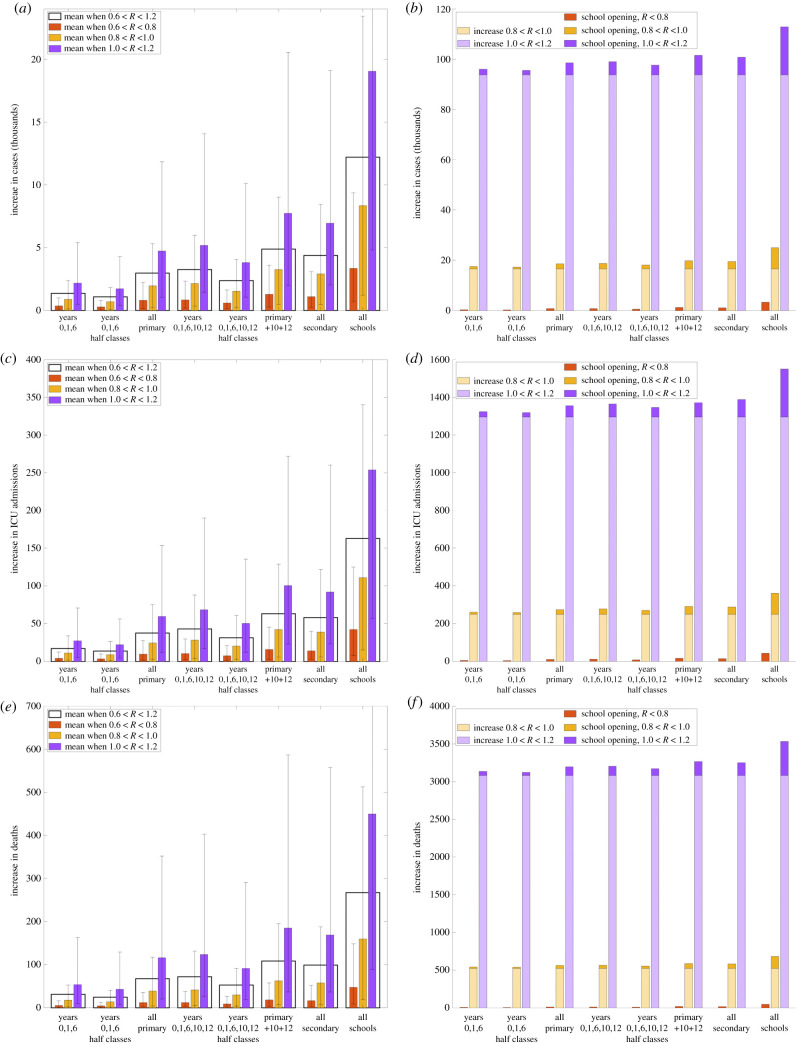
By mid-May 2020, cases of COVID-19 in the UK had been declining for over a month; a multi-phase emergence from lockdown was planned, including a scheduled partial reopening of schools on 1 June 2020. Although evidence suggests that children generally display mild symptoms, the size of the school-age population means the total impact of reopening schools is unclear. Here, we present work from mid-May 2020 that focused on the imminent opening of schools and consider what these results imply for future policy. We compared eight strategies for reopening primary and secondary schools in England. Modifying a transmission model fitted to UK SARS-CoV-2 data, we assessed how reopening schools affects contact patterns, anticipated secondary infections and the relative change in the reproduction number, R. We determined the associated public health impact and its sensitivity to changes in social distancing within the wider community. We predicted that reopening schools with half-sized classes or focused on younger children was unlikely to push R above one. Older children generally have more social contacts, so reopening secondary schools results in more cases than reopening primary schools, while reopening both could have pushed R above one in some regions. Reductions in community social distancing were found to outweigh and exacerbate any impacts of reopening. In particular, opening schools when the reproduction number R is already above one generates the largest increase in cases. Our work indicates that while any school reopening will result in increased mixing and infection amongst children and the wider population, reopening schools alone in June 2020 was unlikely to push R above one. Ultimately, reopening decisions are a difficult trade-off between epidemiological consequences and the emotional, educational and developmental needs of children. Into the future, there are difficult questions about what controls can be instigated such that schools can remain open if cases increase. This article is part of the theme issue 'Modelling that shaped the early COVID-19 pandemic response in the UK'.
Keywords: COVID-19; SARS-CoV-2; deterministic model; mathematical modelling; reopening schools.
Figures
References
-
- Forbes MB, Mehta K, Kumar K, Lu J, Le Saux N, Sampson M, Robinson J. 2020. COVID-19 infection in children: estimating pediatric morbidity and mortality. medRxiv ( 10.1101/2020.05.05.20091751) - DOI
-
- NHS England. 2020. COVID-19 total announced deaths 27 May 2020. https://www.england.nhs.uk/statistics/wp-content/uploads/sites/2/2020/05... [Online] (accessed 23 June 2020).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous