

Performance of plasma kisspeptin as a biomarker for miscarriage improves with gestational age during the first trimester
- PMID: 34053677
- PMCID: PMC8445632
- DOI: 10.1016/j.fertnstert.2021.04.031
Performance of plasma kisspeptin as a biomarker for miscarriage improves with gestational age during the first trimester
Abstract
Objective: To compare the performance of kisspeptin and beta human chorionic gonadotropin (βhCG), both alone and in combination, as biomarkers for miscarriage throughout the first trimester.
Design: Prospective, nested case-control study.
Setting: Tertiary Centre, Queen Charlotte Hospital, London, United Kingdom.
Patient(s): Adult women who had miscarriages (n = 95, 173 samples) and women with healthy pregnancies (n = 265, 557 samples).
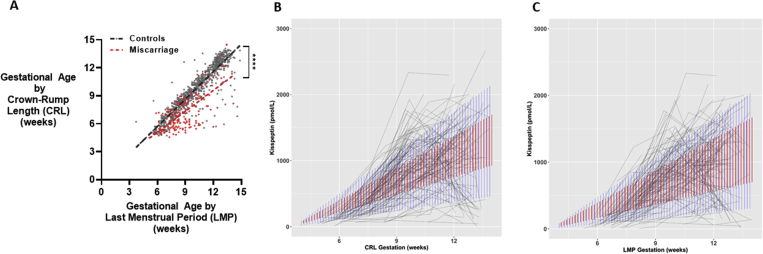
Intervention(s): The participants underwent serial ultrasound scans and blood sampling for measurement of plasma kisspeptin and βhCG levels during the first trimester.
Main outcome measure(s): The ability of plasma kisspeptin and βhCG levels to distinguish pregnancies complicated by miscarriage from healthy pregnancies unaffected by miscarriage.
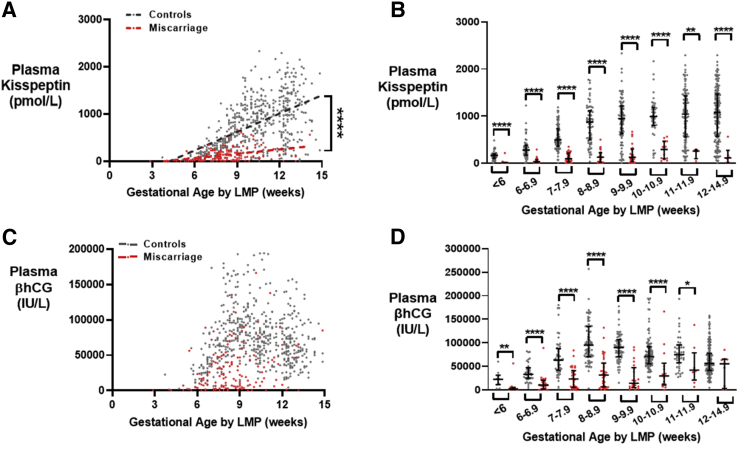
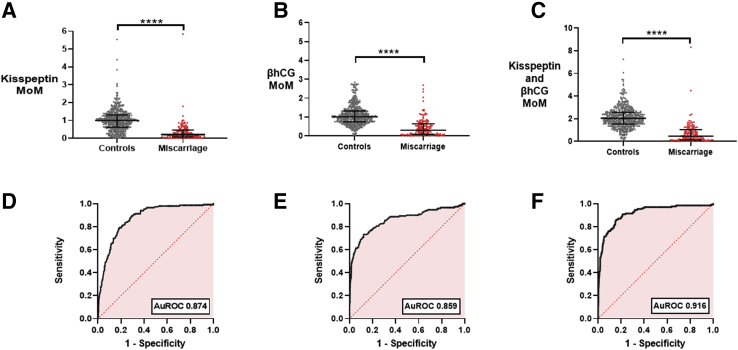
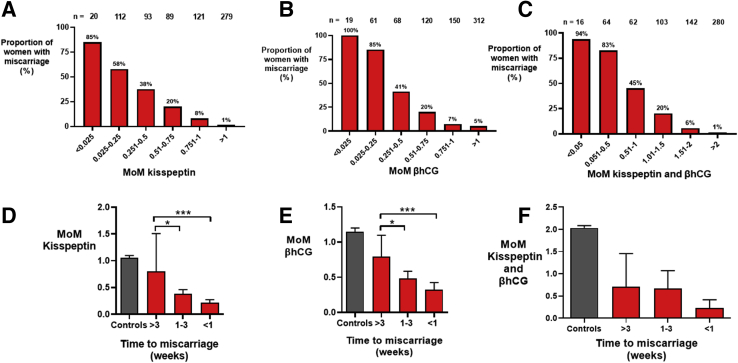
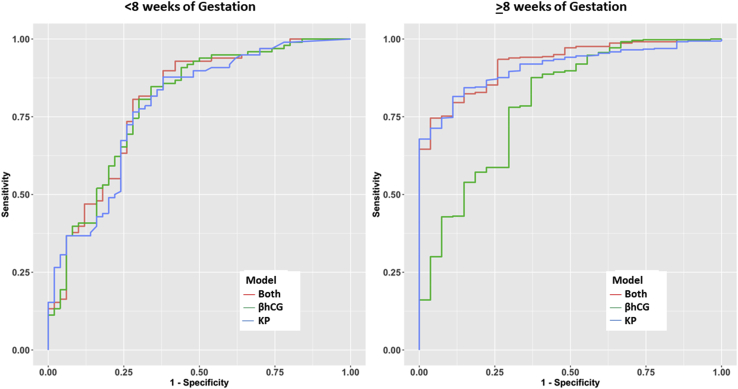
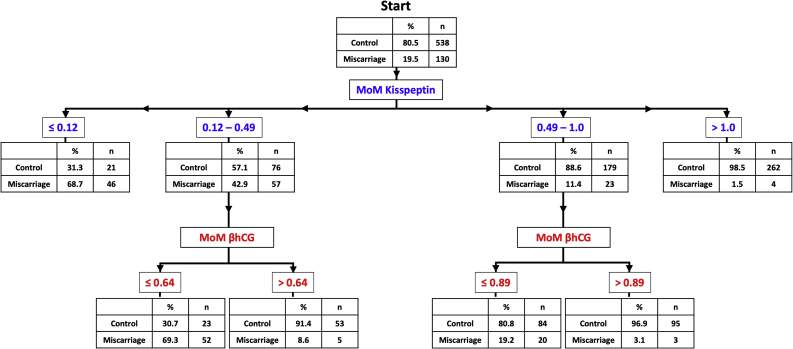
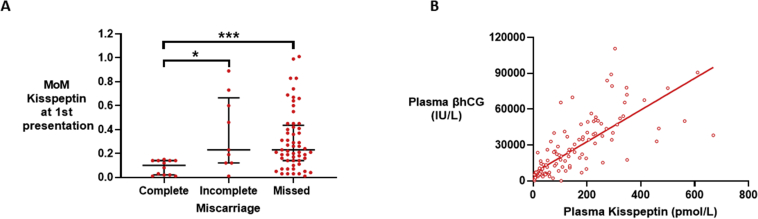
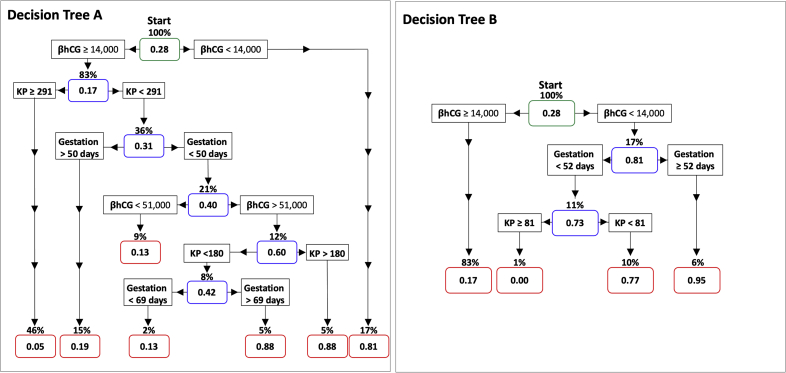
Result(s): Gestation-adjusted levels of circulating kisspeptin and βhCG were lower in samples from women with miscarriages than in women with healthy pregnancies by 79% and 70%, respectively. The area under the receiver-operating characteristic curve for identifying miscarriage during the first trimester was 0.874 (95% confidence interval [CI] 0.844-0.904) for kisspeptin, 0.859 (95% CI 0.820-0.899) for βhCG, and 0.916 (95% CI 0.886-0.946) for the sum of the two markers. The performance of kisspeptin in identifying miscarriage improved with increasing length of gestation, whereas that of βhCG worsened. A decision matrix incorporating kisspeptin, βhCG, and gestational age had 83% to 87% accuracy for the prediction of miscarriage.
Conclusion(s): Plasma kisspeptin is a promising biomarker for miscarriage and provides additional value to βhCG alone, especially during later gestational weeks of the first trimester.
Interpretación de la kisspeptina plasmática como biomarcador de aborto espontáneo mejora con la edad durante el primer trimestre.
Objetivo: Comparar el rendimiento de la kisspeptina y la betagonadotropina coriónica humana (βhCG), tanto solas como en combinación, como biomarcadores de aborto espontáneo durante el primer trimestre.
Diseño: Estudio prospectivo, de casos y controles anidados.
Entorno: Centro terciario, Queen Charlotte Hospital, London, United Kingdom.
Paciente (s): Mujeres adultas que tuvieron abortos espontáneos (n=95. 173 muestras) y mujeres con gestaciones evolutivas (n=265. 557 muestras).
Intervención (es): Las participantes se sometieron a ecografías seriadas y a tomas de muestras de sangre para medir la kisspeptina en plasma y los niveles de βhCG durante el primer trimestre.
Principales medidas de resultado: La capacidad de los niveles plasmáticos de kisspeptina y de la βhCG para distinguir embarazos complicados por aborto espontáneo de embarazos sanos que no se vieron afectados por un aborto espontáneo.
Resultado (s): Los niveles de kisspeptina y de βhCG circulantes ajustados por edad gestacional fueron más bajos en muestras de mujeres con abortos espontáneos que en mujeres con embarazos evolutivos en un 79% y 70%, respectivamente. El área bajo la curva característica de funcionamiento del receptor para la identificación del aborto espontáneo durante el primer trimestre fue de 0,874 (intervalo de confianza [CI] del 95%: 0.844-0.904) para la kisspeptina, 0.859 (CI del 95% 0.820 a 0.899) para la βhCG y 0,916 (CI del 95%: 0,886 a 0,946) para la suma de los dos marcadores. La actuación de kisspeptina en la identificación del aborto espontáneo mejoró con el aumento de la edad gestacional, mientras que la de βhCG empeoró. Una matriz de decisiones incorporando la kisspeptina, la βhCG y la edad gestacional tuvo una precisión del 83% al 87% para la predicción de aborto espontáneo.
Conclusión (es): La kisspeptina plasmática es un biomarcador prometedor para el aborto espontáneo y proporciona un valor adicional a la βhCG sola, especialmente durante las últimas semanas de gestación del primer trimestre.
Keywords: Kisspeptin; miscarriage; pregnancy.
Copyright © 2021 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Kisspeptin, a promising biomarker for miscarriage in early pregnancy.Fertil Steril. 2021 Sep;116(3):672-673. doi: 10.1016/j.fertnstert.2021.06.047. Epub 2021 Aug 5. Fertil Steril. 2021. PMID: 34364674 No abstract available.
References
-
- Royal College of Obstetricians and Gynaecologists. The Management of Early Pregnancy Loss—Green Top Guideline 25; 2006.
-
- Wilcox A.J., Weinberg C.R., O’Connor J.F., Baird D.D., Schlatterer J.P., Canfield R.E. Incidence of early loss of pregnancy. N Engl J Med. 1988;319:189–194. - PubMed
-
- Ammon Avalos L., Galindo C., Li D.K. A systematic review to calculate background miscarriage rates using life table analysis. Birth Defects Res A Clin Mol Teratol. 2012;94:417–423. - PubMed
-
- Soler A., Morales C., Mademont-Soler I., Margarit E., Borrell A., Borobio V. Overview of chromosome abnormalities in first trimester miscarriages: a series of 1,011 consecutive chorionic villi sample karyotypes. Cytogenet Genome Res. 2017;152:81–89. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
